THE STATS ARE BEING SKEWED BY ADDING PNEUMONIA, INFLUENZA AND DEATHS FROM PRE-EXISTING CONDITIONS TO THE COVID DEATH LIST.
STANFORD PHYSICIANS SHOW WHY STATS ARE INSUFFICIENT TO DETERMINE CAUSE OF DEATH.

Birx says government is classifying all deaths of patients with coronavirus as 'COVID-19' deaths, regardless of cause.
The federal government is classifying the deaths of patients infected with the coronavirus as COVID-19 deaths, regardless of any underlying health issues that could have contributed to the loss of someone's life.
Dr. Deborah Birx, the response coordinator for the White House coronavirus task force, said the federal government is continuing to count the suspected COVID-19 deaths, despite other nations doing the opposite.
"There are other countries that if you had a pre-existing condition, and let's say the virus caused you to go to the ICU [intensive care unit] and then have a heart or kidney problem," she said during a Tuesday news briefing at the White House. "Some countries are recording that as a heart issue or a kidney issue and not a COVID-19 death.
"The intent is ... if someone dies WITH COVID-19 we are counting that," she added.
Asked whether the numbers could skew data the government is trying to collect, Birx said that would mostly apply more to rural areas where testing isn't being implemented on a wide scale.
AS MANY HAVE POINTED OUT, DEATH WITH COVID-19 IS NOT DEATH BECAUSE OF THE VIRUS.
GIVEN THIS "DIRECTIVE" BY WHO/CDC, A TERMINALLY ILL CANCER PATIENT ADMITTED TO HOSPITAL, WHO THEN SUCCUMBS TO THE CANCER, BUT TESTS POSITIVE, EVEN POST-MORTEM, FOR COVID-19, CAN BE DECLARED A DEATH BY
C-19.
DITTO FOR A PATIENT WHO DIED OF A MASSIVE CORONARY, A RUPTURED BRAIN ANEURYSM, COMPLETE RENAL FAILURE, ETC.
BUT, NOW, THE HOSPITALS DON'T EVEN HAVE TO TEST. THEY CAN "PRESUME".
THAT CERTAINLY MAKES THE MORTALITY RATE SKYROCKET.
THIS ALSO DOES NOT TAKE INTO ACCOUNT THE UNRELIABILITY OF THE NASAL SWAB TEST THE CDC ALMOST INSISTS ON.
CHINA AND OTHER NATIONS PROVE INFECTION AND CAUSE OF DEATH BY A BLOOD TEST.
NOT IN AMERICA.
APRIL 19, 2020
"Nearly 130,000 confirmed cases of the coronavirus have now been documented in the five boroughs of New York, city statistics revealed on Sunday.
An additional 3,420 diagnoses were made between 2 p.m. Saturday and 1:30 p.m. Sunday, raising the total number to 129,788 — up from 126,368.
The tally of CONFIRMED coronavirus fatalities, meanwhile, rose to 8,811, while the number of “PROBABLE” deaths ATTRIBUTED to the disease hit 4,429, with respective increases of 363 and 165.
COMBINED, the two figures now stand at a staggering 13,240."
WHAT'S "STAGGERING" IS THE IDIOCY OF THIS COMBINING", THIS "PROBABLE|. THIS |ATTRIBUTED" AND "PRESUMED" LOAD OF BS.
SUCH STATS ARE NOT STATS AND THE BUCKET THAT WHO/CDC IS COMBINING THESE IN CAN'T HOLD WATER.
WE MIGHT AS WELL SAY, "WELL, WE PRESUME THEY ALL DIED BECAUSE OF THE WEATHER, PROBABLY, MAYBE, SO WRITE WEATHER AS CAUSE OF DEATH ON THAT DEATH CERTIFICATE. IT'S AS GOOD A GUESS AS ANY."
MUST WONDER...HOW MANY WERE HOSPITALIZED AND DIED IN NEW YORK PER DAY DURING THE ONGOING, STILL WIDESPREAD 2019-2020 FLU SEASON? STANFORD PHYSICIANS SHOW WHY STATS ARE INSUFFICIENT TO DETERMINE CAUSE OF DEATH.
FROM 3,000 TO 10,000 WERE TESTING POSITIVE PER WEEK IN NEW YORK LAST FLU SEASON AND THIS FLU SEASON WAS WORSE, CDC SAYS.
NOT ALL REPORTED COVID-19 DEATHS ARE A RESULT OF THE VIRUS.
Alex Berenson, Apr 3Former NYT reporter and author of 'Tell Your Children',
"As you sit home watching #COVID death counts spiral, please know the official
@CDCgov guidance for coding COVID-related deaths is as follows: any death where the disease “caused or is *assumed* to have caused or *contributed to* death.” Confirmed lab tests are not required.." .

They’re saying U07.1 is now the “catch all”; they don’t specify between primary covid death vs death by other cause *secondary to covid*.
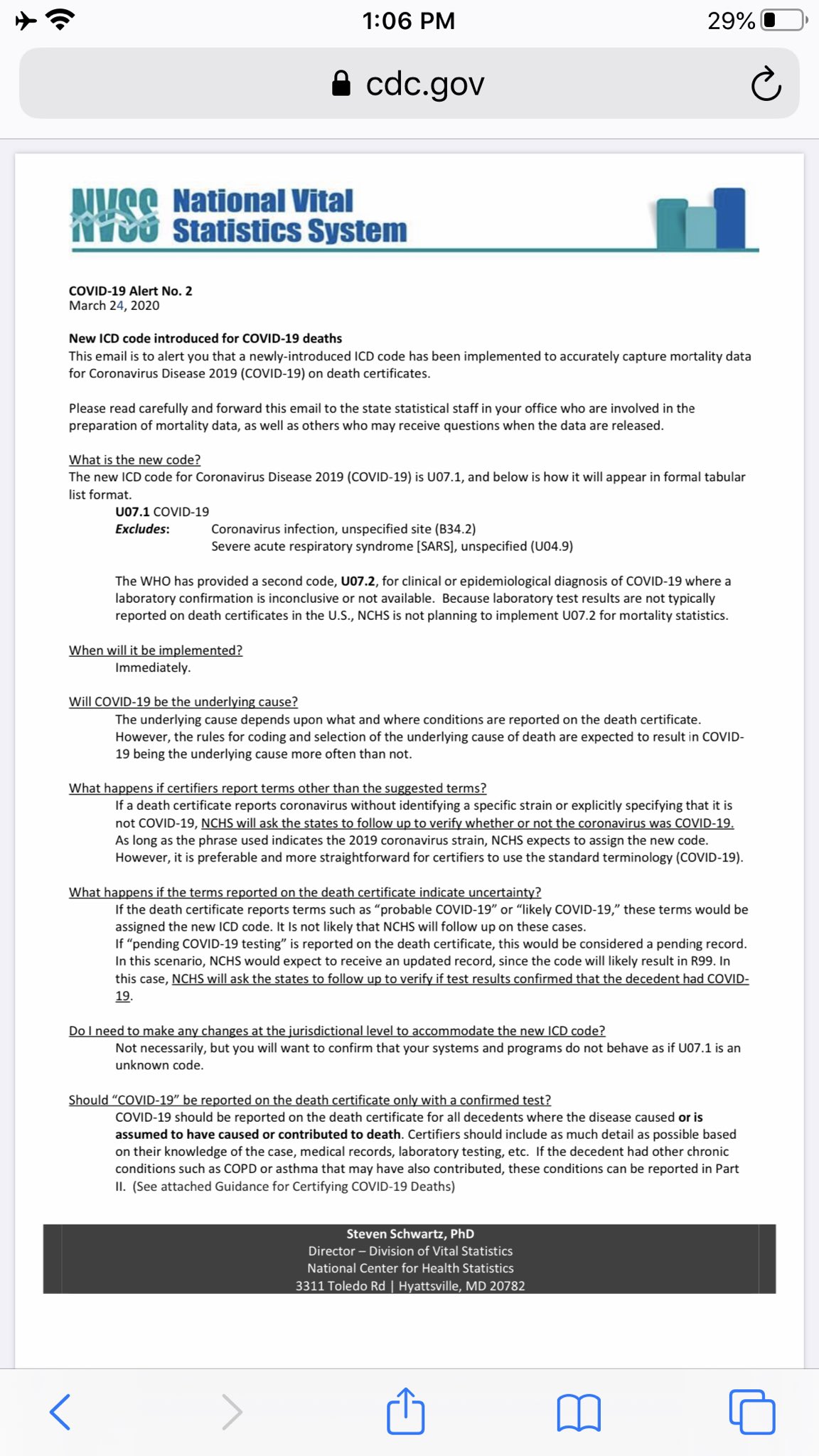
FROM THE CDC WEBSITE, IN PDF:
National Vital Statistics System
COVID-19 Alert No. 2
March 24, 2020
The new ICD code for Cornavirus Disease 2019 UO7.1
"The WHO has provided a second code, U07.2, for clinical or epidemiological diagnosis of COVID-19 where a laboratory confirmation is inconclusive or not available. Because laboratory test results are not typically reported on death certificates in the U.S., NCHS is not planning to implement U07.2 for mortality statistics.
NCHS does not plan to implement UO7.2 for mortality statistics.
"the rules for coding and selection of the underlying cause of death are expected to result in COVID-19 being the underlying cause (of death) more often than not.
THIS WILL GREATLY INCREASE THE NUMBERS OF "COVID-19 DEAD".
FOR EXAMPLE, AN ELDERLY PATIENT ARRIVES WITH A PROBABLE RUPTURING BRAIN ANEURYSM, EXPIRES, IS TESTED POST-MORTEM FOR COVID-19 WITH A POSITIVE RESULT, LEAVING WHOMEVER FILLS OUT DEATH CERTIFICATES TO CHECK THE BOX U07.1.
U07.2 IS NOT BEING IMPLEMENTED, REMEMBER.
NO FURTHER LAB TEST OR DIAGNOSTIC RESULTS ARE REQUIRED OR GIVEN.
PATIENT'S CAUSE OF DEATH BECOMES COVID-19, NOT CEREBRAL HEMORRHAGE.
IS THIS WHY CORVID-19 DEATHS ARE RISING SO QUICKLY?
CDC IS REPORTING ANYONE WHO TESTED POSITIVE FOR COVID-19, AND THEN DIED, AS DEATH BY CORONAVIRUS.
"IT IS POSSIBLE THAT PEOPLE ON THE DEATH LISTS DIED AS A RESULT OF
A PRE-EXISTING CONDITION THEY HAD BEFORE CONTRACTING CORONAVIRUS."
THE STATE OF LOUISIANA, FOLLOWING PROTOCOL, includes anyone who tested positive for COVID-19, and died, in their tally of deaths related to the coronavirus.
It is possible that individuals on the list died as a result of another condition that they had in addition to COVID-19.
40 percent of hospitalized patients with confirmed COVID-19 patients have cardiovascular or cerebrovascular disease.
Jaquan Anderson,age 17, who died in New Orleans Sunday, had tested positive for COVID-19, but the cause and manner of the teen's death remained under investigation.
Anderson’s father, Kevin Moran, said Thursday that he understood his son had died from “heart failure.”
He said he was surprised at the suggestion his son may have died as a result of COVID-19 and disputed that was a certainty.
“It was heart failure,” Moran said. “People don’t want to let you heal. … I’m so upset.”
Anderson’s father, said his son had “not been ill” in the days leading up to his death.
On Wednesday, Los Angeles officials reported what was believed to be the first COVID-19 case in the United States involving a child who tested positive and died.
However, according to media reports, officials said the California child — also 17 — would require additional investigation because “the case was complex and there may be an alternate explanation for this fatality.”
THE BABY THAT RECENTLY DIED IN CONNECTICUT WHO TESTED POSITIVE FOR COVID-19 WAS BROUGHT TO THE HOSPITAL BY AMBULANCE, UNRESPONSIVE AND DECLARED DEAD FROM "POSSIBLE ACCIDENTAL ASPHYXIATION" OR SIDS...SUDDEN INFANT DEATH SYNDROME.
Candace Owens calls for governor to step down after he lied about newborn death link to COVID-19
"The baby arrived unresponsive at a Hartford area hospital and, though the cause of death was unknown when Lamont reacted, the infant reportedly tested positive during a postmortem exam for the virus, which has not normally been seen in otherwise healthy children.
“The death of the infant in Connecticut had nothing to do with COVID-19. I know exactly how the infant died. I know this because people that were involved were mortified and angry, and they were so happy that I spoke out and called out this double-speak. These people reached out to me, not the mother and the father,” Owens said, adding that their account of what happened “completely checks out.”
“I think Governor Ned Lamont should have to step down,” Owens added.
“The post mortem, after this infant had already succumbed, they tested this infant for COVID-19. God knows why,” she said. “Because as I have been trying to shout to you all, it does not matter how you die, they will test you for COVID-19. Then they will use the exact same language that Ned Lamont used: ‘a death linked to COVID-19,’ knowing fully well that the manner in which that infant died had nothing to do with coronavirus.”
“How many more deaths that we are seeing are deaths like this?” Owens asked, pointing to the inaccuracy of figures being “manipulated” to create fear, and demanding to know why journalists are only publishing what politicians tell them."
WHY IS THIS BEING ALLOWED?
HOW CAN PHYSICIANS KNOW WHAT THESE PATIENTS DIED OF WITH NO POST-MORTEMS, NO AUTOPSIES?
HOW CAN WE BE SURE THEY EVEN HAD COVID-19 IF NO LUNG CT SCANS PROVED IT AND ONLY THE INACCURATE CDC TEST WAS USED FOR DIAGNOSIS?
(SEE BELOW ON THAT TEST ACCURACY)
WHAT WOULD ACTUAL DEATH RATES BE IF WE RULE OUT DEATHS FROM SUDDEN HEART ATTACKS IN THE ELDERLY, PRE-EXISTING HEART DISEASE OR LONG-TERM LUNG DISEASE, SIDS, CONGENITAL DEFECTS/ANOMALIES, CANCER?
WHAT WILL THEY COUNT AS COVID DEATHS NEXT, AUTO ACCIDENTS, GUNSHOT WOUNDS, SUICIDES?
LOOKS LIKE WE'LL BE COUNTING FEWER DEATHS! GOOD NEWS!
Key Coronavirus Model Now Predicts Many Fewer U.S. Deaths
A Sunday update of a prominent COVID-19 forecasting model suggests that fewer lives will be lost during the first wave of the coronavirus outbreak than previously thought.
The University of Washington’s Institute for Health Metrics and Evaluation (IHME) now predicts that 81,766 people will die of COVID-19 in the U.S. through early August.
When the model was last updated, on April 2, it predicted 11,765 deaths more deaths, for a total of 93,531.
The change in prediction is due to “a massive infusion of new data,” IHME director Dr. Christopher Murray said in a press release.

The model also revised downward the prediction for the number of ventilators needed at the height of the outbreak. It now predicts the need for 18,992 ventilators, down from 31,782.
One thing that didn’t change between the April 2 and April 5 models is the projected date of the outbreak’s peak. The model still predicts an April 16 apex for the daily COVID-19 death rate. Hospital use is expected to peak on April 15.
BUT ABOUT THOSE QUICK TESTS...THOSE NASAL SWABS...THEY'RE PROVEN INACCURATE.

THE MOST ACCURATE TEST FOR COVID-19 IS A CT SCAN OF THE LUNGS, AS SHOWN ABOVE IN A COVID-POSITIVE PATIENT, BUT THIS IS VERY EXPENSIVE AND IS NOT BEING DONE IN THE U.S. AS MUCH AS IT WAS DONE IN CHINA.
February 26, 2020 — In a study of more than 1,000 patients published in the journal Radiology, chest CT outperformed lab testing in the diagnosis of 2019 novel coronavirus disease (COVID-19). The researchers concluded that CT should be used as the primary screening tool for COVID-19 (also called SARS‐CoV‐2).
In the absence of specific therapeutic drugs or vaccines for COVID-19, it is essential to detect the disease at an early stage and immediately isolate an infected patient from the healthy population.
[SEE ALSO: RADIOLOGICAL PRESENTATION OF CORONAVIRUS ON CT IMAGING]

ABOVE: CLASSIC "GROUND GLASS" OPACITIES OF COVID-19.
A 3-D rendering created from the chest CT scan of a 41-year-old coronavirus patient in China showing ground-glass opacities in several areas of the lungs from the coronavirus pneumonia. This was from one of the first medical imaging studies published on COVID-19 in the journal Radiology.
According to the latest guidelines published by the Chinese government, the diagnosis of COVID-19 must be confirmed by reverse-transcription polymerase chain reaction (RT-PCR) or gene sequencing for respiratory or blood specimens, as the key indicator for hospitalization.
However, with limitations of sample collection and transportation, as well as kit performance, the total positive rate of RT-PCR for throat swab samples has been reported to be about 30 to 60 percent at initial presentation.
In the United States, similar RT-PCR test kits used by the Centers for Disease Control and Prevention (CDC) to test patients and confirm coronavirus infections were cleared for clinical use in the U.S. by an emergency approval by the U.S. Food and Drug Administration (FDA) Jan. 30.
However, when these kits were sent to states, local authorities performed verification testing for quality control and found the tests are not 100 percent accurate, and showed some false negative results.
AS FORBES REPORTED, "The available test is not 100% accurate. Therefore, negative results don’t necessarily preclude an infection. The FDA has stated that the test should be used as one of several tools.
ADD THAT THERE IS NO PROOF OF DEATH BY AUTOPSY.
UNTIL THIS VIRUS OUTBREAK, AUTOPSIES WERE USUALLY PERFORMED TO ASCERTAIN CAUSE OF DEATH.
"Coroner is to perform an autopsy and the results will take several weeks to be communicated to the family."
Autopsies usually take two to four hours to perform. Preliminary results can be released within 24 hours, but the full results of an autopsy may take up to six weeks to prepare.
The College of American Pathologists [CAP] recommends that an autopsy be performed at every death, and experts say that competent autopsies can be beneficial in a wide range of circumstances:
Autopsies are not covered under Medicare, Medicaid or most insurance plans, though some hospitals -- teaching hospitals in particular -- do not charge for autopsies of individuals who passed away in the facility.
A private autopsy by an outside expert can cost between $3,000 and $5,000.
In some cases, there may be an additional charge for the transportation of the body to and from the autopsy facility.
Forensic pathologist Dr. Stephen J. Cina says that autopsies are best if performed within 24 hours of death, before organs deteriorate. Second autopsies have certain limitations because organs have often already been removed and dissected, and the fluids necessary for an evaluation are now no longer available.
AND NOW, MANY NATIONS LIKE ITALY , THE PHILIPPINES AND LIKE INDIA ARE SENDING THE DEAD STRAIGHT TO A CREMATORIUM AND NOT DOING POST-MORTEMS.
NEW YORK IS CONSIDERING DOING THE SAME THING.
FORBES, March 18, 2020
Study: 17.9% Of People With COVID-19 Coronavirus Had No Symptoms
"Both studies reinforce the notion that many people are walking around unaware that they are carrying the virus and potentially spreading it to others. That means just because you
feel well doesn’t mean that you should go out."
The available test is not 100% accurate. Therefore, negative results don’t necessarily preclude an infection. The FDA has stated that the test should be used as one of several tools,
WASHINGTON POST, March 26, 2020
A ‘negative’ coronavirus test result doesn’t always mean you aren’t infected.
No test is 100 percent accurate.
Some test results may incorrectly say that a person has a condition, but they don’t. That’s a false positive.
Other tests may incorrectly say someone doesn’t have a condition, but they do. That’s a false negative, and for covid-19, the illness caused by the coronavirus, at this stage of the outbreak, experts are more worried about this type of inaccuracy.
“If it’s positive … you absolutely can make a [clinical] decision. If it’s negative, you may be early on in the infection and the viral load may be so low you don’t get it,” Anthony S. Fauci, the director of the National Institute for Allergy and Infectious Disease, said in a Q&A with JAMA.
Documentation for the test approved for New York’s state lab explains the possibility of a false positive or false negative, emphasizing that a negative test doesn’t rule out infection.
Another researcher said anecdotal reports peg the genetic coronavirus tests being used in the United States at about 85 percent sensitive.
That means that for someone who has the virus, there’s a 15 percent chance they test negative.
A critical-care blog, EMCrit, estimated that the genetic tests are about 75 percent sensitive and suggests that a single negative swab doesn’t rule out the disease.
“A negative result does not rule out COVID-19 and should not be used as the sole basis for treatment or patient management decisions,” according to the fact sheet for health-care providers. “When diagnostic testing is negative, the possibility of a false negative result should be considered in the context of a patient’s recent exposures and the presence of clinical signs and symptoms consistent with COVID-19."
NOR DOES A POSITIVE TEST MEAN YOU HAVE COVID-19!
HERE'S WHY...FALSE POSITIVES, LIKE FALSE NEGATIVES, ABOUND.
COVID-19 Very Similar to MERS and SARS.
COVID-19 COMES FROM INFECTION WITH THE SARS-CoV2 VIRUS, THE "NOVEL" CORONAVIRUS CAUSING THE PANDEMIC.
COVID-19 is a betacoronavirus, like severe acute respiratory syndrome (SARS) and Middle East respiratory syndrome (MERS), and presenting as viral pneumonia with a wide range of acuity, the bulletin states.
As of Feb. 12, COVID-19 appears to have greater infectivity rate, but a lower case fatality rate, when compared to SARS and MERS.
LOOKING AT THE WHO's DAILY "SITUATION REPORT"
NOTICE HOW MANY NATIONS ARE REPORTING NO DEATHS TO UNDER 100 DEATHS.
NO MEDIA HEADLINES FOR GOOD NEWS.
LOOK AT WHO's "CASE DEFINITIONS":
Case definitions for surveillance
Case and contact definitions are based on the current available information and are regularly revised as new information accumulates.
Countries may need to adapt case definitions depending on their local epidemiological situation and other factors.
All countries are encouraged to publish definitions used online and in regular situation reports, and to document periodic updates to definitions which may affect the interpretation of surveillance data.
Suspect case A.
A patient with acute respiratory illness (fever and at least one sign/symptom of respiratory disease, e.g., cough, shortness of breath), AND a history of travel to or residence in a location reporting community transmission of COVID-19 disease during the 14 days prior to symptom onset;
OR B.
A patient with any acute respiratory illness AND having been in contact with a confirmed or probable COVID-19 case (see definition of contact) in the last 14 days prior to symptom onset;
OR C. A patient with severe acute respiratory illness (fever and at least one sign/symptom of respiratory disease, e.g., cough, shortness of breath; AND requiring hospitalization) AND in the absence of an alternative diagnosis that fully explains the clinical presentation.
[THESE SYMPTOMS ARE IDENTICAL TO COMMON FLU SYMPTOMS AND COULD BE CAUSED BY COMMON FLU, WHICH IS STILL RAMPANT ACROSS AMERICA AND THE GLOBE, AND ARE ALSO THE SYMPTOMS OF BOTH BACTERIAL AND VIRAL PNEUMONIA.]
[ACCORDING TO THE CDC, Other possible serious complications triggered by flu can include inflammation of the heart (myocarditis), brain (encephalitis) or muscle (myositis, rhabdomyolysis) tissues, and multi-organ failure (for example, respiratory and kidney failure).
Flu virus infection of the respiratory tract can trigger an extreme inflammatory response in the body and can lead to sepsis, the body’s life-threatening response to infection.
Flu also can make chronic medical problems worse. For example, people with asthma may experience asthma attacks while they have flu, and people with chronic heart disease may experience a worsening of this condition triggered by flu.
CDC: What are the emergency warning signs of flu?]
Probable case A.
A suspect case for whom testing for the COVID-19 virus is inconclusive;
OR B.
A suspect case for whom testing could not be performed for any reason.
Confirmed case
A person with laboratory confirmation of COVID-19 infection, irrespective of clinical signs and symptoms.
See laboratory guidance for details: https://www.who.int/emergencies/diseases/novel-coronavirus-2019/technicalguidance/laboratory-guidance
https://www.who.int/emergencies/diseases/novel-coronavirus-2019/technical-guidance/laboratory-guidance
If a negative result is obtained from a patient with a high index of suspicion for COVID-19 virus infection, particularly when only upper respiratory tract specimens were collected, additional specimens, including from the lower respiratory tract if possible, should be collected and tested.
To monitor the full extent of the circulation of the virus in the general population, WHO recommends implementing testing for COVID-19 via existing national sentinel surveillance sites for influenza-like illness (ILI) and severe acute respiratory infection (SARI).
Guidance will be made available at: https://www.who.int/emergencies/diseases/novel-coronavirus-2019/technicalguidance/surveillance-and-case-definitions
MEDIA MYTHS, LIES AND SPIN ARE SELDOMLY CORRECTED IN A WAY THAT CALLS PUBLIC ATTENTION TO ANY RARE CORRECTION.
LIKE THESE:
#1 - NO, NEW YORK IS NOT DECIDING WHICH PATIENTS MUST DIE DUE TO A SHORTAGE OF VENTILATORS.
GOVERNOR CUOMO ADMITTED HOSPITALS THERE HAD PLENTY AT THAT TIME.
#2- NO, THOUSANDS OF SURGICAL MASKS WERE NOT STOLEN FROM A NEW YORK HOSPITAL.
THEY FOUND THEM WHERE THEY HAD LEFT THEM.
#3- W.H.O. STATS FOR THE U.S. ARE STILL NOT MATCHING WHAT CDC POSTS.
WHO POSTS CONFIRMED CASES ONLY.
CDC, ON THEIR OWN WEBSITE, STATES THAT
*Data include both confirmed and presumptive positive cases of COVID-19 reported to CDC or tested at CDC since January 21, 2020.
Children stricken with COVID-19 frequently contracted the illness from a family member.
[An unfortunate 'side-effect' of "sheltering in place".]
#4-- NO, A 39-YEAR-OLD WOMAN DID NOT DE IN NEW ORLEANS OF CORONAVIRUS WHILE WAITING FOR TEST RESULTS.
SHE DIDN'T HAVE COVID-19 WHEN HER DOCTOR DID THE FIRST TEST.
A second coronavirus test came back NEGATIVE on Natasha Ott.
We also now know that Ms. Ott had been suffering for two years with an diagnosed intestinal infection.
She was NOT a healthy adult as was previously reported.
The exact reason the woman, Natasha Ott, died remains under investigation by the Coroner’s Office, spokesman Jason Melancon said.
Such investigations can take several weeks to complete.
Ott’s foster sister, Emily Coalson Stamets, has revealed that tests taken both pre- and post-mortem have come back negative for the virus.
Writing today on her own Facebook page she said, ‘When her results came back, they showed that the virus was ‘not detected.’
Note that no coronavirus/COVID-19 test results will say ‘negative’ rather, they will show that the virus was detected or not detected in that particular specimen.’
According to Stamets the doctor who administered Ott’s original test was ‘incredulous’ when the results came through and immediately called LabCorp to have her specimen retested.
She said, ‘The coroner also sent in a specimen to be tested at a local university.’
As of March 25, she wrote, ‘These tests have come back indicating that the coronavirus was ‘not detected.’
AS THE BBC REPORTED 2 DAYS AGO, SWEDEN HAS A LOWER NUMBER OF COVID-19 CASES PER MILLION THAN THE U.S. AND NO, SWEDEN DID NOT SHUT DOWN ITS COUNTRY BECAUSE OF THE PANDEMIC.
YES, SWEDEN'S CLIMATE IS THE TYPE THAT COVID-19 THRIVES IN.
"Sweden Has Lower Number of Coronavirus Cases per Million People than United States -- And Sweden Did Not Shut Down Country or Destroy Its Economy"
Sweden has 239 cases per million people.
The United States has 550 cases per million people.
Sweden remains open for business and life goes on as usual with few restrictions.

The government's strategy here: self-responsibility.
Public health authorities and politicians are still hoping to slow down the spread of the virus without the need for draconian measures.
There are more guidelines than strict rules, with a focus on staying home if you're sick or elderly, washing your hands, and avoiding any non-essential travel, as well as working from home.

Families are able to enjoy the fresh air in a Stockholm park without any restrictions.
Dr. Emma Frans says history will be the judge of which politicians and scientists around Europe have made the best calls so far.
"Nobody really knows what measurements will be the most effective," she says. "I'm quite glad that I'm not the one making these decisions".
COVID-19 cases in America, on March 29, 2020 by CDC:
* Data included both confirmed and presumptive positive cases of COVID-19 reported to CDC or tested at CDC since January 21, 2020
Total cases: 122,653
Total deaths: 2,112
THIS GIVES US A 1.7% DEATH RATE FOR COVID-19.
About 8,500 people are currently hospitalized, in the U.S.
Of those, 2,037 are in intensive care units, which ARE equipped with ventilators.
6.9% OF ALL CURRENT U.S. CASES (122,653) ARE HOSPITALIZED.
ONLY 1.6% OF ALL U.S. CASES NEED TO BE IN ICU.
GLOBALLY, ACCORDING TO W.H.O. ON MARCH 29,2020:
638,146 Confirmed cases.
30,105 Confirmed deaths
(WHO reports only confirmed cases.)
OF 7,774,312,000+ HUMANS ON EARTH, 638,146 HAVE THE NEW CORONAVIRUS.
ISN'T THAT 0.0008% OF THE GLOBAL POPULATION?
A 4.7% DEATH RATE, GLOBALLY.
THERE ARE SOME ODD STATS PUBLISHED BY W.H.O.
WHY HAVE SO FEW FALLEN ILL IN HIGHLY-POPULATED INDIA WHEN THEY ARE PACKED SO CLOSE TOGETHER?
So far, 979 people have tested positive for the coronavirus in India, with 25 dead, according to WHO, 03/29/2020.
SIMILAR LOW NUMBERS FOR VERY CROWDED BANGLADESH AND SINGAPORE.
HOW WELL ARE THEY TESTING THERE?
"120 Million Migrant Workers in India Are Starving and Broke - Walking Hundreds of Miles to Get to Their Homes"
Social distancing is not possible for the poor.
Millions are at risk of starvation, suffering and death due to the lock-down policies.
The poor around the world are the worst hit as jobs are lost and food is scarce.
The panic created by the coronavirus is now injuring and soon will be killing the innocents as third world economies fail.
The poor are being singled out to suffer.

SWINE FLU IS ONGOING IN AMERICA
"Swine flu killed 17,000 people in the US from mid-2009 to mid-2010, including 1,800 children, the U.S. Centers for Disease Control and Prevention reported,.according to REUTERS on FEBRUARY 12, 2010.
"CDC estimates that between 41 million and 84 million cases of 2009 H1N1 occurred between April 2009 and January 16, 2010,” the agency said in a statement. Usually the CDC goes with a middle number, which it puts at about 57 million people infected.
Between 8,330 and 17,160 people died during that time from H1N1, with a middle range of about 12,000, the CDC said.
But between 880 and 1,800 children died, up to 13,000 adults under the age of 65 and only 1,000 to 2,000 elderly.
In a normal flu season, the CDC estimates that 36,000 Americans die of flu, but 90 percent are over the age of 65.
The CDC estimates that 200,000 go into the hospital EVERY YEAR, again mostly frail elderly people with other health conditions.
Do you recall market meltdowns and "OMG, WE'RE ALL GONNA DIE" coverage of pandemic 2009 every single day in fear-mongering headlines like we see daily now?
I don’t.
WERE HOSPITALS SCREAMING THAT THEY COULDN'T HANDLE 200,00 PATIENTS WITHIN A FEW MONTHS TIME FRAME?
NO.
THE FOLLOWING PERTAINS TO H1N1 PATIENTS AND IS FROM W.H.O.:
"Deterioration is rapid, with MANY patients progressing to respiratory failure within 24 hours, requiring immediate admission to an intensive care unit.
Upon admission, most patients need immediate respiratory support with mechanical ventilation."
"MANY PATIENTS."
MANY.
WASHINGTON POST REPORTED THAT IN COVID-19 PATIENTS, 82% HAVE MILD SYMPTOMS.
A study published in February stated that the "death rate" for COVID-19 was 2.3%.
By comparison, the Severe Acute Respiratory Syndrome (SARS) that health experts have likened coronavirus to affected fewer people in 2002–2003, but the death rate was 14–15%, according to the World Health Organization (WHO).
NOT ALL SCHOOLS CLOSED IN 2009-2010
"Schools closed in many states in response to local flu outbreaks.
By April 30, 2009, 300 U.S. schools and school districts had announced closures in response to the outbreak, giving 169,000 students time off.
On May 4, 2009, about 533 schools in just 24 states in the U.S. were closed, affecting about 330,000 students total nationwide.
On September 25, 2009, only 42 schools were closed in eight states as the second wave of the pandemic began.
On May 5, Kathleen Sebelius stated in a CDC news conference that school closures for single confirmed cases of H1N1 influenza were unnecessary, but that parents keep their child home if he or she displays an influenza-like illness.
THE H1N1 FLU WAS ATTACKING THE VERY YOUNG, UNLIKE COVID-19, AND WAS CAUSING A NEW, DEADLY INFECTION OF CHILDRENS' HEARTS THAT WAS QUICKLY FATAL.
BUT NO MANDATORY SCHOOL CLOSINGS IN 2009-2010.
THAT'S CRAZY!
WE LOST ALMOST 2,000 CHILDREN TO H1N1 BACK THEN.
On 7 May 2009, the WHO stated that containment was not feasible and that countries should focus on mitigating the effect of the virus.
They did not recommend closing borders or restricting travel.
WHY ARE THINGS SO DIFFERENT NOW?
THAT SAME SWINE FLU JUST KILLED 34,000 AMERICANS SINCE OCTOBER, 2019 AND IS STILL KILLING AMERICANS!
WHY DIDN'T CDC CLOSE SCHOOLS; WHY WASN'T THE NATION SHUT DOWN AND SENT HOME FOR THAT; AND WHY WEREN'T THE STORE SHELVES BARE , AIRLINES GROUNDED, CRUISES BANNED; WHY WASN'T THE STOCK MARKET CRASHED IN 2009-2010 SWINE FLU/H1N1?
WHY?
2009-2010 PANDEMIC
60.8 million U.S.H1N1 cases (range: 43.3-89.3 million),
274,304 hospitalizations (range 195,086-402,719),
17,000 deaths.
THOSE NUMBERS ARE ALL MUCH LOWER THAN CURRENT NUMBERS FOR 2019-2020 INFLUENZA SEASON, THAT SAME H1N1 THAT WAS DECLARED A PANDEMIC IN 2009 BUT SWEPT ACROSS AMERICA AGAIN THIS SEASON AND IS STILL RAGING RIGHT NOW.
Globally, by 2012, research showed that as many as 579,000 people may have been killed by the disease, as only those fatalities confirmed by laboratory testing were included in the original number, and that many without access to health facilities went uncounted.
The U.S. Public Health Emergency for 2009 H1N1 Influenza expired on June 23, 2010.
On August 10, 2010, the World Health Organization (WHO)
It is likely that the 2009 H1N1 virus will continue to spread for years to come.
0.7–1.4 BILLION WERE INFECTED WORLDWIDE.
THINK LONG ABOUT THOSE STATS.
During our still-widespread 'regular' 2019-2020 flu season, the majority of Americans were again infected by H1N1-09, "Swine Flu", 60.8 MILLION, SO FAR, INFECTED, 274,304 HOSPITALIZED, about 34,000 including 168 children have DIED, so far, AND SOME STILL DYING EACH WEEK.
AND YET BARELY A MAINSTREAM MEDIA WHISPER THAT OUR HOSPITALS WERE SO OVERBURDENED BY SO MANY PATIENTS THAT THEY'D HAVE TO CHOOSE WHICH PATIENTS WOULD DIE, OR THAT WE WOULD RUN OUT OF MEDICAL SUPPLIES, OR THAT MILLIONS MAY STILL HAVE AND BE SPREADING THE H1N1 INFLUENZA AND SHOULD SELF-QUARANTINE, OR THAT WE SHOULD DESTROY THE AMERICAN ECONOMY TO STOP H1N1.
NOW, BYALLTHEGODS, TELL ME WHY.
ANYONE?
WHERE IS THE MEDIA HYSTERIA, OR EVEN MEDIA REPORTS ON THE CURRENT WORSE KILLER, H1N1?
WHY, when in 2009 during THAT pandemic, did we see the start of an economic recovery, but now we are having an economic collapse?
Washington Post, Mach 10, 2020:
"The Strategic National Stockpile, which is the federal government's cache of drugs and medical supplies, distributed 85 million N95 face masks in response to the H1N1 influenza pandemic in 2009, and has not significantly refilled them since that time industry and health experts say."
WHY NOT?
DIDN'T THEY LEARN ANYTHING FROM THE BIG SWINE FLU SCARE?
THEY WERE WARNED SINCE 2009 TO RESTOCK.
"There have been warnings about the potential shortages for years. In mid-2009, the International Safety Equipment Association, a trade group for makers of protective equipment, urged that the N95 masks be restocked, warning of "significant shortages" if there was another pandemic.
The next year, the Association of State and Territorial Health Officials, a nonprofit representing public health agencies also called for the masks to be replenished.
NPR (NATIONAL PUBLIC RADIO), ARTICLE ON VENTILATORS, March 14, 2020:
The latest study available estimates there are about 62,000 ventilators in hospitals nationwide. That figure is seven years old — so the actual number could be higher.
There are also some machines in federally stockpiled emergency supplies, though the exact number isn't public.
"There is a strategic national stockpile of ventilators, but the numbers are classified," says Toner. It's been "publicly stated," he says, that there are about 10,000 ventilators in the national stockpile. "That number might be a bit outdated, but it's probably about right," he says.
WRONG, WRONG, WRONG!
WE HAVE OVER 162,000 VENTILATORS AVAILABLE RIGHT NOW.
NEW YORK TIMES, 4 DAYS AFTER NPR's LOW GUESS:
March 18, 2020
Hospitals in the United States have roughly 160,000 ventilators. There are a further 12,700 in the National Strategic Stockpile, a cache of medical supplies maintained by the federal government.
MEDIA BIAS AND MEDIA SPIN
Friday, Jan 31, 2020, a few weeks before Coronavirus had officially spread to other countries (which led to the bad stock market week Feb 24-Feb 28), the Trump Administration announced travel restrictions on China.
Politico and others blasted and condemned Trump for his order.
Politico on 2/4/20: "The Trump admin's quarantine and travel ban in response to the Wuhan coronavirus could UNDERCUT international efforts to fight the outbreak by antagonizing Chinese leaders, as well as stigmatizing people of Asian descent, according to public health experts and lawmakers."
DO NOTE THAT BACK THEN POLITICO AND ALL MSM WERE CALLING IT THE 'WUHAN VIRUS', YET THEY'D SOON DAMN TRUMP FOR SAYING THAT.
MAINSTREAM MEDIA HEADLINES RECENTLY ABOUT NEW YORK's GOVERNOR CUOMO'S REQUEST FOR MORE VENTILATORS
HERE'S THE TRUTH:In an interview with NBC's Lester Holt, New York Governor Andrew Cuomo said he hopes the state doesn’t need 30,000 ventilators, but that he determined the need based “on the numbers and on the science.”
Gov. Andrew Cuomo Admits Stockpile of Thousands of Unused VentilatorsCuomo responded to a comment from President Donald Trump on Twitter that there were thousands of ventilators in New York not being used.
THE W.H.O. HAS STATED THAT 80% OF THOSE INFECTED BY COVID-19 WILL HAVE MILD CASES.
"According to W.H.O the virus will cause a mild respiratory infection in about 80% of those infected, about half will have pneumonia and another 15% will develop severe illness with at least 5% needing critical care.
W.H.O stresses that fundamental public health interventions can still help to limit the spread and drive down cases of transmission even in areas where it is spreading rapidly as the work from authorities in China, Singapore, and South Korea are showing."
WHAT IS THE POPULATION OF NEW YORK STATE? 19.44 million
IF THE ENTIRE STATE, EVERY MAN, WOMAN AND CHILD, CONTRACTED COVID-19, IF 15% OF THEM WERE SEVERE, 2,916,000, AND IF 5% OF THOSE, 145,800, REQUIRED INTENSIVE CARE AND NEEDED A VENTILATOR, THEN, YES, CUOMO MIGHT NEED OVER 140,000 VENTILATORS.
AND, SURPRISE! WE HAVE CURRENTLY ABOUT 170,000 VENTILATORS AVAILABLE TODAY, WITH MORE BEING MADE RIGHT NOW.
The U.S. currently has an estimated 160,000 ventilators.
These incredibly complex machines cost upward of $50,000 apiece, and involve international supply chains.
FROM A PDF TITLED "VENTILATOR STOCKPILING AND AVAILABILITY IN THE US AND INTERNATIONALLY":
US acute care hospitals own approximately 62,000 full-feature mechanical ventilators.
Calculations suggest that around 28,883 of these ventilators (46.4%) can be used to ventilate pediatric and neonatal patients.
The study also reported an additional 98,000 ventilators that are not full-featured but can still provide basic function.
• Based on these numbers, the maximum number that can be potentially ventilated is around 160,000.
• US: 20.5 ICU beds with mechanical ventilation capability per 100,000 population
• Canada: 8.7 ICU beds with mechanical ventilation capability per 100,000 population
• Australia & New Zealand: 5.4 ICU beds with mechanical ventilation capability per 100,000 population
These numbers suggest that the capacity of other countries to provide ventilation therapy might be significantly lower than our own.
In addition, the CDC Strategic National Stockpile has an estimated 8,900 ventilators as of 2010.(OVER 12,000 as of this year).
[SEE ALSO: Ajao A, Nystrom SV, Koonin LM, et al. Assessing the capacity of the US health care system to use additional mechanical ventilators during a large-scale public health emergency. Disaster Med Public Health Prep 2015;9(6):634-641]
DOING THE MATH,
62,000 FULL-FEATURED IN HOSPITALS NOW.
98,000 ADDITIONAL NON-FULL-FEATURED
12,000 IN NATIONAL STOCKPILE
170,000.
Ventilators are stored and kept as managed inventory.
Malatino et al report that shipments from managed inventory “could arrive within 24-36 hours of the federal decision to deploy them.”
NEW YORK TIMES, 4 DAYS AFTER NPR's LOW GUESS:
March 18, 2020
Hospitals in the United States have roughly 160,000 ventilators. There are a further 12,700 in the National Strategic Stockpile, a cache of medical supplies maintained by the federal government.
MEDIA BIAS AND MEDIA SPIN
Friday, Jan 31, 2020, a few weeks before Coronavirus had officially spread to other countries (which led to the bad stock market week Feb 24-Feb 28), the Trump Administration announced travel restrictions on China.
Politico and others blasted and condemned Trump for his order.
Politico on 2/4/20: "The Trump admin's quarantine and travel ban in response to the Wuhan coronavirus could UNDERCUT international efforts to fight the outbreak by antagonizing Chinese leaders, as well as stigmatizing people of Asian descent, according to public health experts and lawmakers."
DO NOTE THAT BACK THEN POLITICO AND ALL MSM WERE CALLING IT THE 'WUHAN VIRUS', YET THEY'D SOON DAMN TRUMP FOR SAYING THAT.
MAINSTREAM MEDIA HEADLINES RECENTLY ABOUT NEW YORK's GOVERNOR CUOMO'S REQUEST FOR MORE VENTILATORS
HERE'S THE TRUTH:In an interview with NBC's Lester Holt, New York Governor Andrew Cuomo said he hopes the state doesn’t need 30,000 ventilators, but that he determined the need based “on the numbers and on the science.”
Gov. Andrew Cuomo Admits Stockpile of Thousands of Unused VentilatorsCuomo responded to a comment from President Donald Trump on Twitter that there were thousands of ventilators in New York not being used.
“Yes, they’re in a stockpile because that’s where they are supposed to be, because we don’t need them yet,” Cuomo said. “We need them for the apex, the apex isn’t here, so we’re gathering them in a stockpile.”
Cuomo’s comments demonstrate there is not an immediate shortage in ventilators in the city, despite alarming reports.
“We don’t need them today, because we’re not at capacity today, that’s why they’re not deployed because they’re not needed,” Cuomo said.
In an interview on Fox News on Thursday night, Trump appeared skeptical that New York would need 40,000 ventilators.
“I have a feeling that a lot of the numbers that are being said in some areas are just bigger than they’re going to be,” he said.
THE W.H.O. HAS STATED THAT 80% OF THOSE INFECTED BY COVID-19 WILL HAVE MILD CASES.
"According to W.H.O the virus will cause a mild respiratory infection in about 80% of those infected, about half will have pneumonia and another 15% will develop severe illness with at least 5% needing critical care.
W.H.O stresses that fundamental public health interventions can still help to limit the spread and drive down cases of transmission even in areas where it is spreading rapidly as the work from authorities in China, Singapore, and South Korea are showing."
WHAT IS THE POPULATION OF NEW YORK STATE? 19.44 million
IF THE ENTIRE STATE, EVERY MAN, WOMAN AND CHILD, CONTRACTED COVID-19, IF 15% OF THEM WERE SEVERE, 2,916,000, AND IF 5% OF THOSE, 145,800, REQUIRED INTENSIVE CARE AND NEEDED A VENTILATOR, THEN, YES, CUOMO MIGHT NEED OVER 140,000 VENTILATORS.
AND, SURPRISE! WE HAVE CURRENTLY ABOUT 170,000 VENTILATORS AVAILABLE TODAY, WITH MORE BEING MADE RIGHT NOW.
The U.S. currently has an estimated 160,000 ventilators.
These incredibly complex machines cost upward of $50,000 apiece, and involve international supply chains.
FROM A PDF TITLED "VENTILATOR STOCKPILING AND AVAILABILITY IN THE US AND INTERNATIONALLY":
US acute care hospitals own approximately 62,000 full-feature mechanical ventilators.
Calculations suggest that around 28,883 of these ventilators (46.4%) can be used to ventilate pediatric and neonatal patients.
The study also reported an additional 98,000 ventilators that are not full-featured but can still provide basic function.
• Based on these numbers, the maximum number that can be potentially ventilated is around 160,000.
• US: 20.5 ICU beds with mechanical ventilation capability per 100,000 population
• Canada: 8.7 ICU beds with mechanical ventilation capability per 100,000 population
• Australia & New Zealand: 5.4 ICU beds with mechanical ventilation capability per 100,000 population
These numbers suggest that the capacity of other countries to provide ventilation therapy might be significantly lower than our own.
In addition, the CDC Strategic National Stockpile has an estimated 8,900 ventilators as of 2010.(OVER 12,000 as of this year).
[SEE ALSO: Ajao A, Nystrom SV, Koonin LM, et al. Assessing the capacity of the US health care system to use additional mechanical ventilators during a large-scale public health emergency. Disaster Med Public Health Prep 2015;9(6):634-641]
DOING THE MATH,
62,000 FULL-FEATURED IN HOSPITALS NOW.
98,000 ADDITIONAL NON-FULL-FEATURED
12,000 IN NATIONAL STOCKPILE
170,000.
Ventilators are stored and kept as managed inventory.
Malatino et al report that shipments from managed inventory “could arrive within 24-36 hours of the federal decision to deploy them.”
The authors go on to describe the multi step process for requesting additional ventilators from the CDC Strategic National Stockpile.
The US Department of Health and Human Services (HHS) estimates that 865,000 US residents would be hospitalized during a moderate pandemic (as in 1957 and 1968) and 9.9 million during a severe pandemic (as in 1918).
Moderate (1958/68-like) = 64,875 would need mechanical ventilation
Severe (1918-like) = 742,500 would need mechanical ventilation
FACE MASKS ARE BEING MADE DAILY.
Mar. 25, 2020
"Another major company is stepping up to help the fight against COVID-19.
MyPillow, the Minnesota manufacturer of specialty pillows, linens, and other household products, says that it is answering the call for more face masks as the country continues to deal with the global coronavirus pandemic.
The company Tweeted that it is making face masks for hospitals across the country. MyPillow joins a growing list of private companies pitching in to address the shortage of face masks.
Companies including 3M and Honeywell are set to manufacture millions of additional N95 respirator masks to protect doctors, nurses and other health care workers who are treating patients with coronavirus."
WHEN THE CHIPS ARE DOWN, PEOPLE RALLY TO DELIVER WHAT'S NEEDED.
OUR GOVERNMENTS COULD TAKE LESSONS FROM 'COMMON FOLKS'.
AND THEN THERE'S THE HOARDERS... Labor Union SEIU Found Hoarding 39 Million Face Masks
March 27, 2020
SEIU miraculously “found” 39 million medical face masks in its warehouses three days after U.S. Attorney General Bill Barr announced that the feds were going to start going after hoarders.
“If you have a big supply of toilet paper in your house, this is not something you have to worry about. But if you are sitting on a warehouse with masks, surgical masks, you will be hearing a knock on your door,” Barr added.
On Monday, March 23, Trump signed an executive order giving the Department of Justice the task of prosecuting hoarders.
Per NBC San Francisco:
"Service Employees International Union United Healthcare Workers West announced Thursday that it located 39 million N95 masks and will make them available to state and local governments and health care systems that are fighting the novel coronavirus outbreak.
The union found a distributor with the masks, which are cleared for surgical use, after pleas from health care workers as new coronavirus cases surge across the state and the country as a whole.
Union officials said they also found a supplier that can produce some 20 million protective masks per week and another that can supply millions of protective face shields."
INNOVATION IN TIME OF CRISIS
March 29, 2020
Brussels (AFP) - As hospitals face an overload of COVID-19 patients struggling to breathe, innovative medical staff are turning to snorkeling masks from sports stores to stop their lungs collapsing.
Endo Tools Therapeutics, whose know-how in 3D printing for medical use has proved invaluable.
"They are to be used for patients with severe respiratory problems. The aim is to avoid having to intubate the trachea of the patient and put them on a respirator," said Frederic Bonnier, a respiratory physiotherapist at the hospital who also teaches at the university.
He spearheaded the design of a custom-made valve that fits to the top of full-face masks, where the snorkel is meant to go, allowing them to connect to standard BiPAP machines that feed pressurised air into masks.
This helps prevent the collapse of alveoli, lung air sacs needed for the intake of oxygen into our bodies and the exhalation of carbon dioxide. Pneumonia brought on by COVID-19 inflames the lung membrane and fills those sacs with liquid.
The snorkeling mask solution could be a stop-gap measure for patients on the brink of intensive-care treatment but for whom no beds nor respirators are available. Hospital masks for the less-intensive BiPAP (bi-level positive airway pressure) machines are also lacking.
Bonnier said that from Monday he will testing 50 of the masks on patients.
They are the same brand as those used by Italian doctors, donated by the French sportswear retailer Decathlon that has stores worldwide. The masks themselves are made in Italy."
CREATING CHAOS?
2009 SWINE FLU PANDEMIC.
"In January 2010, Wolfgang Wodarg, a German deputy who trained as a physician and now chairs the health committee at the Council of Europe, claimed major firms had organized a "campaign of panic" to put pressure on the World Health Organization (WHO) to declare a "false pandemic" to sell vaccines.
Wodarg said the WHO's "false pandemic" flu campaign is "one of the greatest medicine scandals of the century." He said that the "false pandemic" campaign began in May 2009 in Mexico City, when a hundred or so "normal" reported influenza cases were declared to be the beginning of a threatening new pandemic, although he said there was little scientific evidence for it.
Nevertheless, he argued that the WHO, "in cooperation with some big pharmaceutical companies and their scientists, re-defined pandemics," removing the statement that "an enormous amount of people have contracted the illness or died" from its existing definition and replacing it by stating simply that there has to be a virus, spreading beyond borders and to which people have no immunity.
The WHO responded by stating that they take their duty to provide independent advice seriously and guarded against interference from outside interests. Announcing a review of the WHO's actions, spokeswoman Fadela Chaib stated: "Criticism is part of an outbreak cycle. We expect and indeed welcome criticism and the chance to discuss it".
In March 2010, the Council of Europe launched an inquiry into "the influence of the pharmaceutical companies on the global swine flu campaign", and a preliminary report is in preparation.
On 12 April 2010, Keiji Fukuda, the WHO's top influenza expert, stated that the system leading to the declaration of a pandemic led to confusion about H1N1 circulating around the world and he expressed concern that there was a failure to communicate in regard to uncertainties about the new virus, which turned out to be not as deadly as feared.
WHO Director-General Margaret Chan appointed 29 flu experts from outside the organization to conduct a review of WHO's handling of the H1N1 flu pandemic. She told them, "We want a frank, critical, transparent, credible and independent review of our performance."
In June 2010, Fiona Godlee, editor-in-chief of the BMJ (British Medical Journal), published an editorial which criticized the WHO, saying that an investigation had disclosed that some of the experts advising WHO on the pandemic had financial ties with drug companies which were producing antivirals and vaccines.
Margaret Chan, Director-General of the WHO, replied stating, "Without question, the BMJ feature and editorial will leave many readers with the impression that WHO's decision to declare a pandemic was at least partially influenced by a desire to boost the profits of the pharmaceutical industry."
AND NOW?
WELL, WE NEED MORE WHISTLEBLOWERS.
AND TRUTH.
AND COMMON SENSE.
BUT NO FEAR.
//WW
No comments:
Post a Comment