
JUST AS MANY PHYSICIANS AND EXPERTS ARE SAYING, NO EXCESS COVID DEATHS.
YES, MORE TESTS...TESTS THAT MAY BE FALSE POSITIVE, BUT NO CLIMB IN THE DEATH RATE FROM COVID.
THE DATA SHOWS THE LIES GOVERNMENTS AND MAINSTREAM MEDIA ARE USING TO CREATE A NEW ROUND OF UNNECESSARY LOCKDOWNS.
WHAT THEY'RE DOING IS MEDICALLY UNETHICAL, ILLEGAL AND NATION-DESTROYING.
PCR TESTS RULED UNRELIABLE, ILLEGALLY USED FOR QUARANTINE.
Nov 20, 2020
An appeals court in Portugal has ruled that the PCR process is not a reliable test for Sars-Cov-2, and therefore any enforced quarantine based on those test results is unlawful.
Further, the ruling suggested that any forced quarantine applied to healthy people could be a violation of their fundamental right to liberty.
This very important legal decision faces total media blackout in the Western world, especially in the U.S. where, since day 1, ANYONE who has gone against the acceptable narrative have been
WHY NOT REPORT IT? IT'S BIG NEWS!
In their ruling, judges Margarida Ramos de Almeida and Ana Paramés referred to several scientific studies. Most notably this study by Jaafar et al., which found that – when running PCR tests with 35 cycles or more – the accuracy dropped to 3%, meaning up to 97% of positive results could be false positives.
The ruling goes on to conclude that, based on the science they read, any PCR test using over 25 cycles is totally unreliable.
Even fearmonger-in-chief Anthony Fauci has publicly stated anything over 35 is totally unusable.You can read the complete ruling in the original Portuguese here, and translated into English here.
The media reaction to this case has been entirely predictable – they have not mentioned it. At all. Anywhere.
The ruling was published on November 11th, and has been referenced by many "alt-news sites" since…but the mainstream outlets are maintaining a complete blackout on it.
You can see a NON-GOOGLE search for headlines, articles that I did by clicking on the search link below.
NOT ONE REPORT BY ANY MAINSTREAM MEDIA, ZERO, NONE.
https://duckduckgo.com/?q=An+appeals+court+in+Portugal+has+ruled+that+the+PCR+process+is+not+a+reliable+test+for+Sars-Cov-2%2C&atb=v221-6rj&ia=web
NO COVID-19 EXCESS DEATHS. DAILY MORTALITY RATE DATA READS NORMAL, OR EVEN LOWER SOME MONTHS.
Michael Yeadon, Ph.D., former vice-president and chief scientific adviser for 16 years of the drug company Pfizer, reveals the COVID-19 'scam' and challenges anyone who doesn't believe him to seek out any database on total mortality.
"If you do that, you will find that the daily death count is absolutely bang-on normal," Yeadon says.
For some months, the death count is actually slightly lower than the average norm over the past five years.
"So, what we're seeing now is a natural death rate — about 1,700 people die each day in the U.K. in any given year," Yeadon says — but many of these deaths are now falsely attributed to COVID-19. "I'm calling out the statistics, and even the claim that there is an ongoing pandemic, as false," he says.
And, he adds, "You cannot have a lethal pandemic stalking the land and not have excess deaths."
Yeadon currently is founder and CEO of the biotech company Ziarco, now owned by Novartis.
In an open letter to the British health minister, Yeadon wrote:
"I have read the consultation document. I've rarely been as shocked and upset. All vaccines against the SARS-COV-2 virus are by definition novel. No candidate vaccine has been in development for more than a few months. If any such vaccine is approved for use under any circumstances that are not EXPLICITLY experimental, I believe that recipients are being misled to a criminal extent.
This is because there are precisely zero human volunteers for whom there could possibly be more than a few months past-dose safety information. My concern does not arise because I have negative views about vaccines (I don't).
Instead, it's the very principle that politicians seem ready to waive that new medical interventions at this, incomplete state of development, should not be made available to subjects on anything other than an explicitly experimental basis. That's my concern.
And the reason for that concern is that it is not known what the safety profile will be, six months or a year or longer after dosing. You have literally no data on this and neither does anyone else.
It isn't that I'm saying that unacceptable adverse effects will emerge after longer intervals after dosing. No: it is that you have no idea what will happen yet, despite this, you'll be creating the impression that you do …
I don't trust you. You've not been straightforward and have behaved appallingly throughout this crisis. You're still doing it now, misleading about infection risk from young children. Why should I believe you in relation to experimental vaccines?" British journalist Anna Brees interviewed Yeadon and that is available online at https://youtu.be/vL1-oVMM8rk ."
In the interview, he discusses several concerns, including his belief that widespread PCR testing is creating the false idea that the pandemic is resurging, as the total mortality rate is completely normal.
Speaking with Julia Hartley-Brewer, Dr. Yeadon said the Government is "using a test with an undeclared false positive rate. That's dreadful. If you don't know what it is - shame on you."
Dr. Yeadon wants those who have tested positive for coronavirus to be tested again to eliminate the possibility of the test being a false positive.
Dr. Carl Hennigan, professor of Evidence Based Medicine at Oxford agrees with Yeadon.
The Tea Room posted just yesterday that the FDA has finally admitted these tests are PRONE TO FALSE POSITIVE RESULTS.
The New York Times Aug 29, 2020, wrote: "Tests authorized by the F.D.A. provide only a yes-no answer to infection, and will identify as positive patients with low amounts of virus in their bodies.
Some of the nation’s leading public health experts are raising a new concern in the endless debate over coronavirus testing in the United States: The standard tests are diagnosing huge numbers of people who may be carrying relatively insignificant amounts of the virus.
Most of these people are not likely to be contagious, and identifying them may contribute to bottlenecks that prevent those who are contagious from being found in time. But similar PCR tests for other viruses do offer some sense of how contagious an infected patient may be: The results may include a rough estimate of the amount of virus in the patient’s body.
“We’ve been using one type of data for everything, and that is just plus or minus — that’s all,” Dr. Mina said. “We’re using that for clinical diagnostics, for public health, for policy decision-making.” But yes-no isn’t good enough, he added. It’s the amount of virus that should dictate the infected patient’s next steps. “It’s really irresponsible, I think, to forgo the recognition that this is a quantitative issue,” Dr. Mina said.
The PCR test amplifies genetic matter from the virus in cycles; the fewer cycles required, the greater the amount of virus, or viral load, in the sample. The greater the viral load, the more likely the patient is to be contagious.
This number of amplification cycles needed to find the virus, called the cycle threshold, is never included in the results sent to doctors and coronavirus patients, although it could tell them how infectious the patients are.
In three sets of testing data that include cycle thresholds, compiled by officials in Massachusetts, New York and Nevada, up to 90 percent of people testing positive carried barely any virus, a review by The Times found.
On one Thursday, the United States recorded 45,604 new coronavirus cases, according to a database maintained by The Times. If the rates of contagiousness in Massachusetts and New York were to apply nationwide, then perhaps only 4,500 of those people may actually need to isolate and submit to contact tracing.
One solution would be to adjust the cycle threshold used now to decide that a patient is infected. Most tests set the limit at 40, a few at 37. This means that you are positive for the coronavirus if the test process required up to 40 cycles, or 37, to detect the virus.
Tests with thresholds so high may detect not just live virus but also genetic fragments, leftovers from infection that pose no particular risk — akin to finding a hair in a room long after a person has left, Dr. Mina said. Any test with a cycle threshold above 35 is too sensitive, agreed Juliet Morrison, a virologist at the University of California, Riverside. “I’m shocked that people would think that 40 could represent a positive,” she said.
A more reasonable cutoff would be 30 to 35, she added. Dr. Mina said he would set the figure at 30, or even less. Those changes would mean the amount of genetic material in a patient’s sample would have to be 100-fold to 1,000-fold that of the current standard for the test to return a positive result — at least, one worth acting on.
“It’s just kind of mind-blowing to me that people are not recording the C.T. values from all these tests, that they’re just returning a positive or a negative,” Angela Rasmussen, a virologist at Columbia University in New York said.
The C.D.C.’s own calculations suggest that it is extremely difficult to detect any live virus in a sample above a threshold of 33 cycles. Officials at some state labs said the C.D.C. had not asked them to note threshold values or to share them with contact-tracing organizations.
Officials at the Wadsworth Center, New York’s state lab, have access to C.T. values from tests they have processed, and analyzed their numbers at The Times’s request. In July, the lab identified 872 positive tests, based on a threshold of 40 cycles.
With a cutoff of 35, about 43 percent of those tests would no longer qualify as positive. About 63 percent would no longer be judged positive if the cycles were limited to 30.
In Massachusetts, from 85 to 90 percent of people who tested positive in July with a cycle threshold of 40 would have been deemed negative if the threshold were 30 cycles, Dr. Mina said. “I would say that none of those people should be contact-traced, not one,” he said.
Dr. Ashish Jha, director of the Harvard Global Health Institute. “Boy, does it really change the way we need to be thinking about testing.”
Dr. Jha said he had thought of the PCR test as a problem because it cannot scale to the volume, frequency or speed of tests needed. “But what I am realizing is that a really substantial part of the problem is that we’re not even testing the people who we need to be testing,” he said.
But with 20 percent or more of people testing positive for the virus in some parts of the country, Dr. Mina and other researchers are questioning the use of PCR tests as a frontline diagnostic tool.
People infected with the virus are most infectious from a day or two before symptoms appear till about five days after. But at the current testing rates, “you’re not going to be doing it frequently enough to have any chance of really capturing somebody in that window,” Dr. Mina added.
These deaths may be characterized as being COVID related, but that's only because they have been falsely lumped into that category due to false positives being recorded within 28 days of death.
Again, people are being tested very regularly, and the rate of false positives is extremely high. All hospital patients are also tested upon admission, so when they die — regardless of the cause — they're likely to have a false positive on their record, which then lumps them into the death tally for COVID-19.
"The longer you stay in hospital, the more likely you are to die, obviously," Yeadon says. "You would be released if you were well and improving. So … long-stay patients are both more likely to die statistically, and much more likely to be tested so often that they'll have a false positive test.
That is what I think is happening … It's a convenience for someone playing some macabre game, because I don't think it's an error anymore … I've spoken to people in [public health] and they're embarrassed that they're not even being allowed to characterize and publish the information you would need to know to work out how useful the test is. That's not being done."
Since COVID-19 first began circulating within the United States, public health officials have known that those with underlying medical conditions face higher risks for severe illness and death if they contract the disease. A recent report from the CDC appears to drill down that point with striking numbers, showing that 94% of U.S. deaths involving COVID-19 since February were also associated with other conditions, or comorbidities.
As I have shown before, according to the CDC's own web page: "For 6% of [coronavirus disease 2019] deaths, COVID-19 was the only cause mentioned. For deaths with conditions or causes in addition to COVID-19, on average, there were 2.6 additional conditions or causes per death. The number of deaths with each condition or cause is shown for all deaths and by age groups."
In an interview last week Dr. Yeadon was asked:
“we are basing a government policy, an economic policy, a civil liberties policy, in terms of limiting people to six people in a meeting…all based on, what may well be, completely fake data on this coronavirus?”
Dr. Yeadon answered with a simple “yes.”
Dr. Yeadon said in the interview that, given the “shape” of all important indicators in a worldwide pandemic, such as hospitalizations, ICU utilization, and deaths, “the pandemic is fundamentally over.”
Yeadon said in the interview:
“Were it not for the test data that you get from the TV all the time, you would rightly conclude that the pandemic was over, as nothing much has happened. Of course people go to the hospital, moving into the autumn flu season…but there is no science to suggest a second wave should happen.”
In a paper published this month, which was co-authored by Yeadon and two of his colleagues, “How Likely is a Second Wave?”, the scientists write:
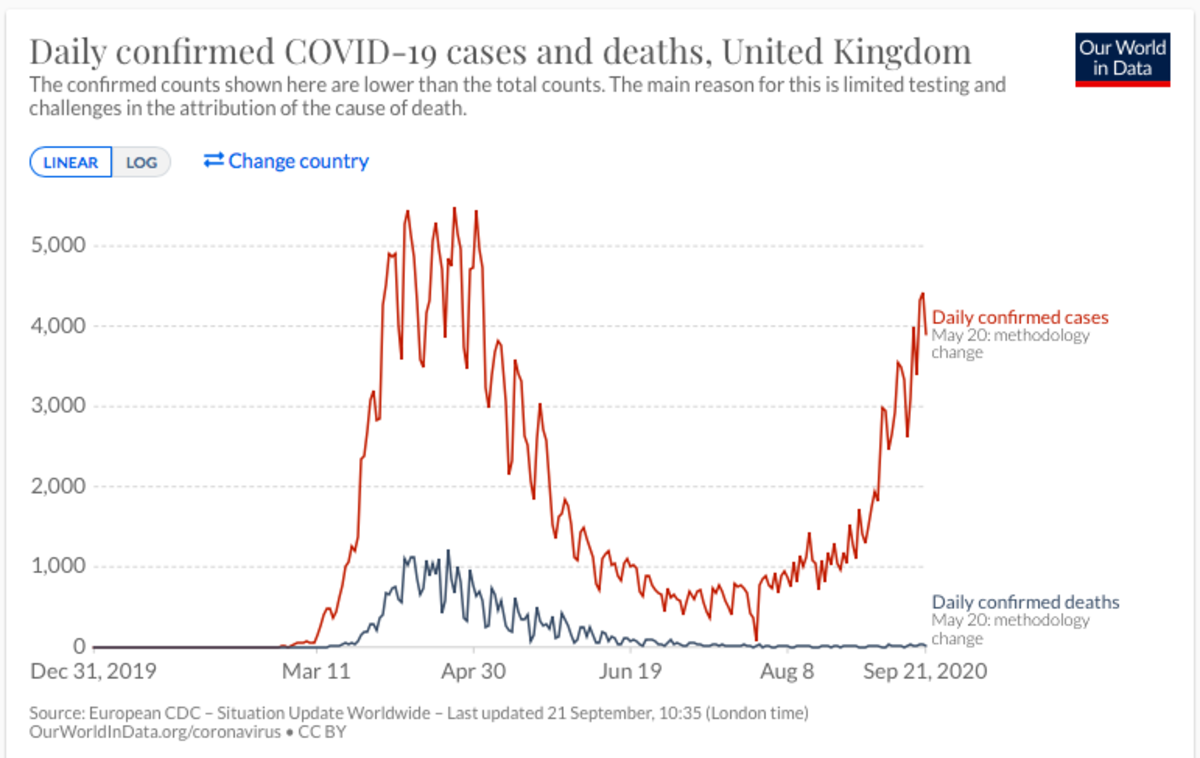
“It has widely been observed that in all heavily infected countries in Europe and several of the US states likewise, that the shape of the daily deaths vs. time curves is similar to ours in the UK. Many of these curves are not just similar, but almost super imposable.”
In the data for UK, Sweden, the US, and the world, it can be seen that in all cases, deaths were on the rise in March through mid or late April, then began tapering off in a smooth slope which flattened around the end of June and continues to today. The case rates however, based on testing, rise and swing upwards and downwards wildly.
(SEE CHARTS AT TOP OF PAGE.)
AS A CANCER PATIENT WITH CONGESTIVE HEART FAILURE, I HAVE HAD ALL OF MY VISITS PUT ON HOLD EXCEPT ONE ULTRASOUND LOOKING FOR BLOOD CLOTS.
HOW MANY LIKE ME HAVEN'T BEEN AS FORTUNATE AND DIED WAITING FOR THESE TREATMENTS AND PROCEDURES?
I HAD TO GO BY AMBULANCE TO THE EMERGENCY ROOM JUST TO BE SEEN FOR MY LOW OXYGEN SATURATION, 89%, OUTRAGEOUS HEART PALPITATIONS, INABILITY TO GET ONE GOOD, DEEP BREATH.
HAD I NOT GONE WHEN I DID, I ABSOLUTELY BELIEVE I WOULD HAVE DIED WHILE WAITING TO SEE MY CARDIOLOGIST.
WAS I ADMITTED? NO.
EVEN THOUGH I WAS RECENTLY RELEASED FROM QUARANTINE AFTER A SECOND POSITIVE TEST, MAKING TWO QUARANTINES SINCE MAY FOR COVID-19, I WAS SENT HOME, TOLD I'D BE SAFER THERE.
THIS WHOLE THING HAS BEEN CHAOS AND CONFUSION, MAYBE PURPOSELY SO.
THE CDC FAILED, THE WHO FAILED, THE FDA FAILED, MAINSTREAM MEDIA FED THE MASS HYSTERIA AND HERE WE ARE, LOOKING AT THE SECOND TRY TO BRING AMERICA AND OTHER NATIONS DOWN, TO REDUCE US ALL TO TERRIFIED, UNQUESTIONING, COMPLIANT SHEEP, FOLLOWING THE CALL OF THE WOLF-SHEPHERDS.
"HEAR AND OBEY! DO AS WE SAY! ...OR ELSE..."
MEANWHILE, ECONOMIES LIE IN RUIN, MORE SUICIDES, FAMILIES LOSING EVERYTHING, BUSINESSES CLOSING FOREVER...THE BLEAKNESS OF OUR FUTURE IS TORMENTING.
IT IS WEDNESDAY, NOVEMBER 25, 2020, THE DAY BEFORE THANKSGIVING IN AMERICA AND MILLIONS ARE TOO DAMNED SCARED TO HAVE THANKSGIVING MEALS WITH LOVED ONES.
"HIDE, HIDE IN FEAR! BE AFRAID, SAVE YOURSELVES!" WE'RE TOLD REPEATEDLY.
WHAT WILL WE DO?
HEAR AND OBEY?
NOT MY HOUSE!
This very important legal decision faces total media blackout in the Western world, especially in the U.S. where, since day 1, ANYONE who has gone against the acceptable narrative have been
WHY NOT REPORT IT? IT'S BIG NEWS!
In their ruling, judges Margarida Ramos de Almeida and Ana Paramés referred to several scientific studies. Most notably this study by Jaafar et al., which found that – when running PCR tests with 35 cycles or more – the accuracy dropped to 3%, meaning up to 97% of positive results could be false positives.
The ruling goes on to conclude that, based on the science they read, any PCR test using over 25 cycles is totally unreliable.
Governments and private labs have been very tight-lipped about the exact number of cycles they run when PCR testing, but it is known to sometimes be as high as 45.
Even fearmonger-in-chief Anthony Fauci has publicly stated anything over 35 is totally unusable.You can read the complete ruling in the original Portuguese here, and translated into English here.
The media reaction to this case has been entirely predictable – they have not mentioned it. At all. Anywhere.
The ruling was published on November 11th, and has been referenced by many "alt-news sites" since…but the mainstream outlets are maintaining a complete blackout on it.
You can see a NON-GOOGLE search for headlines, articles that I did by clicking on the search link below.
NOT ONE REPORT BY ANY MAINSTREAM MEDIA, ZERO, NONE.
https://duckduckgo.com/?q=An+appeals+court+in+Portugal+has+ruled+that+the+PCR+process+is+not+a+reliable+test+for+Sars-Cov-2%2C&atb=v221-6rj&ia=web
NO COVID-19 EXCESS DEATHS. DAILY MORTALITY RATE DATA READS NORMAL, OR EVEN LOWER SOME MONTHS.
Michael Yeadon, Ph.D., former vice-president and chief scientific adviser for 16 years of the drug company Pfizer, reveals the COVID-19 'scam' and challenges anyone who doesn't believe him to seek out any database on total mortality.
"If you do that, you will find that the daily death count is absolutely bang-on normal," Yeadon says.
For some months, the death count is actually slightly lower than the average norm over the past five years.
"So, what we're seeing now is a natural death rate — about 1,700 people die each day in the U.K. in any given year," Yeadon says — but many of these deaths are now falsely attributed to COVID-19. "I'm calling out the statistics, and even the claim that there is an ongoing pandemic, as false," he says.
And, he adds, "You cannot have a lethal pandemic stalking the land and not have excess deaths."
Yeadon currently is founder and CEO of the biotech company Ziarco, now owned by Novartis.
In an open letter to the British health minister, Yeadon wrote:
"I have read the consultation document. I've rarely been as shocked and upset. All vaccines against the SARS-COV-2 virus are by definition novel. No candidate vaccine has been in development for more than a few months. If any such vaccine is approved for use under any circumstances that are not EXPLICITLY experimental, I believe that recipients are being misled to a criminal extent.
This is because there are precisely zero human volunteers for whom there could possibly be more than a few months past-dose safety information. My concern does not arise because I have negative views about vaccines (I don't).
Instead, it's the very principle that politicians seem ready to waive that new medical interventions at this, incomplete state of development, should not be made available to subjects on anything other than an explicitly experimental basis. That's my concern.
And the reason for that concern is that it is not known what the safety profile will be, six months or a year or longer after dosing. You have literally no data on this and neither does anyone else.
It isn't that I'm saying that unacceptable adverse effects will emerge after longer intervals after dosing. No: it is that you have no idea what will happen yet, despite this, you'll be creating the impression that you do …
I don't trust you. You've not been straightforward and have behaved appallingly throughout this crisis. You're still doing it now, misleading about infection risk from young children. Why should I believe you in relation to experimental vaccines?" British journalist Anna Brees interviewed Yeadon and that is available online at https://youtu.be/vL1-oVMM8rk ."
In the interview, he discusses several concerns, including his belief that widespread PCR testing is creating the false idea that the pandemic is resurging, as the total mortality rate is completely normal.
He also discusses his concerns about COVID-19 vaccine mandates.
There are currently no excess deaths in the daily mortality counts while Covid "cases" increase.
MOST of those "cases" should NOT be listed as cases, since they are NOT hospitalized and many remain ASYMPTOMATIC.
Mortality data show many deaths are mainly due to heart disease, stroke and cancer, which suggests they are deaths caused by lack of routine medical care due to the pandemic restrictions
The deaths we see are primarily people aged 45 to 65, with equal distribution between the sexes, who had pre-existing conditions.
Yeadon reissued his challenge to the Health Secretary Matt Hancock regarding the coronavirus testing.
There are currently no excess deaths in the daily mortality counts while Covid "cases" increase.
MOST of those "cases" should NOT be listed as cases, since they are NOT hospitalized and many remain ASYMPTOMATIC.
Mortality data show many deaths are mainly due to heart disease, stroke and cancer, which suggests they are deaths caused by lack of routine medical care due to the pandemic restrictions
The deaths we see are primarily people aged 45 to 65, with equal distribution between the sexes, who had pre-existing conditions.
Yeadon reissued his challenge to the Health Secretary Matt Hancock regarding the coronavirus testing.
Speaking with Julia Hartley-Brewer, Dr. Yeadon said the Government is "using a test with an undeclared false positive rate. That's dreadful. If you don't know what it is - shame on you."
Dr. Yeadon wants those who have tested positive for coronavirus to be tested again to eliminate the possibility of the test being a false positive.
Dr. Carl Hennigan, professor of Evidence Based Medicine at Oxford agrees with Yeadon.
The Tea Room posted just yesterday that the FDA has finally admitted these tests are PRONE TO FALSE POSITIVE RESULTS.
The New York Times Aug 29, 2020, wrote: "Tests authorized by the F.D.A. provide only a yes-no answer to infection, and will identify as positive patients with low amounts of virus in their bodies.
Some of the nation’s leading public health experts are raising a new concern in the endless debate over coronavirus testing in the United States: The standard tests are diagnosing huge numbers of people who may be carrying relatively insignificant amounts of the virus.
Most of these people are not likely to be contagious, and identifying them may contribute to bottlenecks that prevent those who are contagious from being found in time. But similar PCR tests for other viruses do offer some sense of how contagious an infected patient may be: The results may include a rough estimate of the amount of virus in the patient’s body.
“We’ve been using one type of data for everything, and that is just plus or minus — that’s all,” Dr. Mina said. “We’re using that for clinical diagnostics, for public health, for policy decision-making.” But yes-no isn’t good enough, he added. It’s the amount of virus that should dictate the infected patient’s next steps. “It’s really irresponsible, I think, to forgo the recognition that this is a quantitative issue,” Dr. Mina said.
The PCR test amplifies genetic matter from the virus in cycles; the fewer cycles required, the greater the amount of virus, or viral load, in the sample. The greater the viral load, the more likely the patient is to be contagious.
This number of amplification cycles needed to find the virus, called the cycle threshold, is never included in the results sent to doctors and coronavirus patients, although it could tell them how infectious the patients are.
In three sets of testing data that include cycle thresholds, compiled by officials in Massachusetts, New York and Nevada, up to 90 percent of people testing positive carried barely any virus, a review by The Times found.
On one Thursday, the United States recorded 45,604 new coronavirus cases, according to a database maintained by The Times. If the rates of contagiousness in Massachusetts and New York were to apply nationwide, then perhaps only 4,500 of those people may actually need to isolate and submit to contact tracing.
One solution would be to adjust the cycle threshold used now to decide that a patient is infected. Most tests set the limit at 40, a few at 37. This means that you are positive for the coronavirus if the test process required up to 40 cycles, or 37, to detect the virus.
Tests with thresholds so high may detect not just live virus but also genetic fragments, leftovers from infection that pose no particular risk — akin to finding a hair in a room long after a person has left, Dr. Mina said. Any test with a cycle threshold above 35 is too sensitive, agreed Juliet Morrison, a virologist at the University of California, Riverside. “I’m shocked that people would think that 40 could represent a positive,” she said.
A more reasonable cutoff would be 30 to 35, she added. Dr. Mina said he would set the figure at 30, or even less. Those changes would mean the amount of genetic material in a patient’s sample would have to be 100-fold to 1,000-fold that of the current standard for the test to return a positive result — at least, one worth acting on.
“It’s just kind of mind-blowing to me that people are not recording the C.T. values from all these tests, that they’re just returning a positive or a negative,” Angela Rasmussen, a virologist at Columbia University in New York said.
The C.D.C.’s own calculations suggest that it is extremely difficult to detect any live virus in a sample above a threshold of 33 cycles. Officials at some state labs said the C.D.C. had not asked them to note threshold values or to share them with contact-tracing organizations.
Officials at the Wadsworth Center, New York’s state lab, have access to C.T. values from tests they have processed, and analyzed their numbers at The Times’s request. In July, the lab identified 872 positive tests, based on a threshold of 40 cycles.
With a cutoff of 35, about 43 percent of those tests would no longer qualify as positive. About 63 percent would no longer be judged positive if the cycles were limited to 30.
In Massachusetts, from 85 to 90 percent of people who tested positive in July with a cycle threshold of 40 would have been deemed negative if the threshold were 30 cycles, Dr. Mina said. “I would say that none of those people should be contact-traced, not one,” he said.
Dr. Ashish Jha, director of the Harvard Global Health Institute. “Boy, does it really change the way we need to be thinking about testing.”
Dr. Jha said he had thought of the PCR test as a problem because it cannot scale to the volume, frequency or speed of tests needed. “But what I am realizing is that a really substantial part of the problem is that we’re not even testing the people who we need to be testing,” he said.
But with 20 percent or more of people testing positive for the virus in some parts of the country, Dr. Mina and other researchers are questioning the use of PCR tests as a frontline diagnostic tool.
People infected with the virus are most infectious from a day or two before symptoms appear till about five days after. But at the current testing rates, “you’re not going to be doing it frequently enough to have any chance of really capturing somebody in that window,” Dr. Mina added.
These deaths may be characterized as being COVID related, but that's only because they have been falsely lumped into that category due to false positives being recorded within 28 days of death.
Again, people are being tested very regularly, and the rate of false positives is extremely high. All hospital patients are also tested upon admission, so when they die — regardless of the cause — they're likely to have a false positive on their record, which then lumps them into the death tally for COVID-19.
"The longer you stay in hospital, the more likely you are to die, obviously," Yeadon says. "You would be released if you were well and improving. So … long-stay patients are both more likely to die statistically, and much more likely to be tested so often that they'll have a false positive test.
That is what I think is happening … It's a convenience for someone playing some macabre game, because I don't think it's an error anymore … I've spoken to people in [public health] and they're embarrassed that they're not even being allowed to characterize and publish the information you would need to know to work out how useful the test is. That's not being done."
Since COVID-19 first began circulating within the United States, public health officials have known that those with underlying medical conditions face higher risks for severe illness and death if they contract the disease. A recent report from the CDC appears to drill down that point with striking numbers, showing that 94% of U.S. deaths involving COVID-19 since February were also associated with other conditions, or comorbidities.
As I have shown before, according to the CDC's own web page: "For 6% of [coronavirus disease 2019] deaths, COVID-19 was the only cause mentioned. For deaths with conditions or causes in addition to COVID-19, on average, there were 2.6 additional conditions or causes per death. The number of deaths with each condition or cause is shown for all deaths and by age groups."
In an interview last week Dr. Yeadon was asked:
“we are basing a government policy, an economic policy, a civil liberties policy, in terms of limiting people to six people in a meeting…all based on, what may well be, completely fake data on this coronavirus?”
Dr. Yeadon answered with a simple “yes.”
Dr. Yeadon said in the interview that, given the “shape” of all important indicators in a worldwide pandemic, such as hospitalizations, ICU utilization, and deaths, “the pandemic is fundamentally over.”
Yeadon said in the interview:
“Were it not for the test data that you get from the TV all the time, you would rightly conclude that the pandemic was over, as nothing much has happened. Of course people go to the hospital, moving into the autumn flu season…but there is no science to suggest a second wave should happen.”
In a paper published this month, which was co-authored by Yeadon and two of his colleagues, “How Likely is a Second Wave?”, the scientists write:
“It has widely been observed that in all heavily infected countries in Europe and several of the US states likewise, that the shape of the daily deaths vs. time curves is similar to ours in the UK. Many of these curves are not just similar, but almost super imposable.”
In the data for UK, Sweden, the US, and the world, it can be seen that in all cases, deaths were on the rise in March through mid or late April, then began tapering off in a smooth slope which flattened around the end of June and continues to today. The case rates however, based on testing, rise and swing upwards and downwards wildly.
(SEE CHARTS AT TOP OF PAGE.)
More than 600 doctors signed a letter in May urging President Trump to end the nationwide coronavirus shutdowns and referred to orders issued by states that keep businesses closed as a “mass casualty incident” with devastating consequences.
The letter points out the negative consequences that doctors have observed since state governments started issuing their stay-at-home orders, including patients missing checkups with doctors, increases in substance abuse and alcohol abuse, and negative financial implications, according to Fox News.
WHAT DOCTORS AND MEDIA HAVE NOT POINTED OUT IS HOW MANY PROCEDURES AND TREATMENTS FOR THOSE WITH PRE-EXISTING CONDITIONS HAVE BEEN CANCELLED,AS A CANCER PATIENT WITH CONGESTIVE HEART FAILURE, I HAVE HAD ALL OF MY VISITS PUT ON HOLD EXCEPT ONE ULTRASOUND LOOKING FOR BLOOD CLOTS.
HOW MANY LIKE ME HAVEN'T BEEN AS FORTUNATE AND DIED WAITING FOR THESE TREATMENTS AND PROCEDURES?
I HAD TO GO BY AMBULANCE TO THE EMERGENCY ROOM JUST TO BE SEEN FOR MY LOW OXYGEN SATURATION, 89%, OUTRAGEOUS HEART PALPITATIONS, INABILITY TO GET ONE GOOD, DEEP BREATH.
HAD I NOT GONE WHEN I DID, I ABSOLUTELY BELIEVE I WOULD HAVE DIED WHILE WAITING TO SEE MY CARDIOLOGIST.
WAS I ADMITTED? NO.
EVEN THOUGH I WAS RECENTLY RELEASED FROM QUARANTINE AFTER A SECOND POSITIVE TEST, MAKING TWO QUARANTINES SINCE MAY FOR COVID-19, I WAS SENT HOME, TOLD I'D BE SAFER THERE.
THIS WHOLE THING HAS BEEN CHAOS AND CONFUSION, MAYBE PURPOSELY SO.
THE CDC FAILED, THE WHO FAILED, THE FDA FAILED, MAINSTREAM MEDIA FED THE MASS HYSTERIA AND HERE WE ARE, LOOKING AT THE SECOND TRY TO BRING AMERICA AND OTHER NATIONS DOWN, TO REDUCE US ALL TO TERRIFIED, UNQUESTIONING, COMPLIANT SHEEP, FOLLOWING THE CALL OF THE WOLF-SHEPHERDS.
"HEAR AND OBEY! DO AS WE SAY! ...OR ELSE..."
MEANWHILE, ECONOMIES LIE IN RUIN, MORE SUICIDES, FAMILIES LOSING EVERYTHING, BUSINESSES CLOSING FOREVER...THE BLEAKNESS OF OUR FUTURE IS TORMENTING.
IT IS WEDNESDAY, NOVEMBER 25, 2020, THE DAY BEFORE THANKSGIVING IN AMERICA AND MILLIONS ARE TOO DAMNED SCARED TO HAVE THANKSGIVING MEALS WITH LOVED ONES.
"HIDE, HIDE IN FEAR! BE AFRAID, SAVE YOURSELVES!" WE'RE TOLD REPEATEDLY.
WHAT WILL WE DO?
HEAR AND OBEY?
NOT MY HOUSE!



//WW
No comments:
Post a Comment