HEADLINE TODAY, AUG. 12, 2020:
The confirmed number of coronavirus cases in the world has reached 20 million.
Shock, awe, fear, trembling, right?
NO.
SOME ARE TRYING TO COMPARE CV-19 TO THE SPANISH FLU.
NOT EVEN CLOSE!
The 1918 Spanish Flu is generally believed to have infected 500 MILLION and killed more than 50 MILLION people worldwide, the world's population being only
1.8 BILLION at that time.
Some researchers have estimated a death rate as high as 10 to 20%.
During World War I in Europe, the flu struck troops and civilians in the spring of 1918 and it flared up later in the U.S., where 675,000 people died.
Then a second round swept the globe in the Fall of 1918.
"What's remarkable is this was contagious enough that it appears to have landed in places for which there's no apparent contact," Nancy Bristow, a history professor at the University of Puget Sound in Tacoma, Wash., told NPR, citing an Inuit village in Alaska, where 72 out of 80 residents died from the 1918 flu over the course of five days.
"The 1918 pandemic was the most severe pandemic that we have on record," said Amesh Adalja, an infectious disease physician and senior scholar at the Johns Hopkins Center for Health Security. "We had no ICUs at that time. We had no antivirals, had no vaccines for flu. We had no idea that the flu was even a virus at that time."
SO, NO, MEDIA FEAR MONGERS, DON'T DARE COMPARE CV-19 TO SPANISH FLU! COMPARE IT TO THE SHAM-SCAM OF THE 2009 'PANDEMIC'.
20 million COVID-19 cases in a world of almost 8 billion (7.8 billion) humans so far with 11,109,443 of those in 'The Americas'?
That's far fewer than the number of "normal" flu cases each year in just America.
BOTH the 'Asian Flu' in 1957-1958 and the 'Hong Kong Flu' in 1968-1969, infected 500 MILLION worldwide and killed an estimated 1-4 MILLION humans.
The 2009 'Flu Pandemic' infected 0.7 to 1.4 BILLION but killed "only" 151,700–575,400.
THAT was another MAJOR SCARE CAMPAIGN in the mainstream media.
The 2009 flu was of the SAME type as th Spanish Flu...H1N1.
In the 2019-2020 flu season, America has had an estimated 45 MILLION flu cases.An estimated 24,000 to 62,000 have died.
That number includes 187 children, to date.
And CDC stopped posting numbers back in April.
751,154 CV-19 deaths worldwide since DECEMBER 2019 compared to 50 MILLION to 100 MILLION during the Spanish Flu?
LUDICROUS COMPARISON!
HOW MANY OF THOSE COUNTED CV-19 DEATHS COULD THEY PROVE BY AUTOPSY?
Flu Kills up to 646,000 People Worldwide Each Year
BUT, the updated flu numbers do NOT include deaths during flu pandemics, when even more are usually infected and even more die.
WHY NOT?
The United States, India and Brazil have together accounted for nearly two-thirds of all COVID-19 cases since the world hit 15 million on July 22.
WHY are the U.S. numbers so high?
THE U.S. NUMBER OF CV-19 CASES IS QUITE LOW COMPARED TO A SEASONAL KILLER WE ALL SEE EACH YEAR...INFLUENZA.
In 2017-2018 approximately 45 MILLION Americans were infected by the FLU.
"HIGH" estimates put that number at about 58 MILLION Americans...
JUST Americans.
Depending on which news agency you read, between 46,000 – 95,000 Americans died that flu season. This info comes from the CDC.
According to new estimates published today, between 291,000 and 646,000 people worldwide die from seasonal influenza-related respiratory illnesses each year, higher than a previous estimate of 250,000 to 500,000 and based on a robust, multinational survey.
The new estimate, from a collaborative study by CDC and global health partners, appears today in The Lancet.
The estimate excludes deaths during pandemics.
WHY?
“These findings remind us of the seriousness of flu and that flu prevention should really be a global priority,” says Joe Bresee, M.D., associate director for global health in CDC’s Influenza Division and a study co-author.
The new estimates use more recent data, taken from a larger and more diverse group of countries than previous estimates. Forty-seven countries contributed to this effort. Researchers calculated annual seasonal influenza-associated respiratory deaths for 33 of those countries (57 percent of the world’s population) that had death records and seasonal influenza surveillance information for a minimum of four years between 1999 and 2015. Statistical modeling with those results was used to generate an estimate of the number of flu-associated respiratory deaths for 185 countries across the world.
BELOW, U.S. ONLY CHART
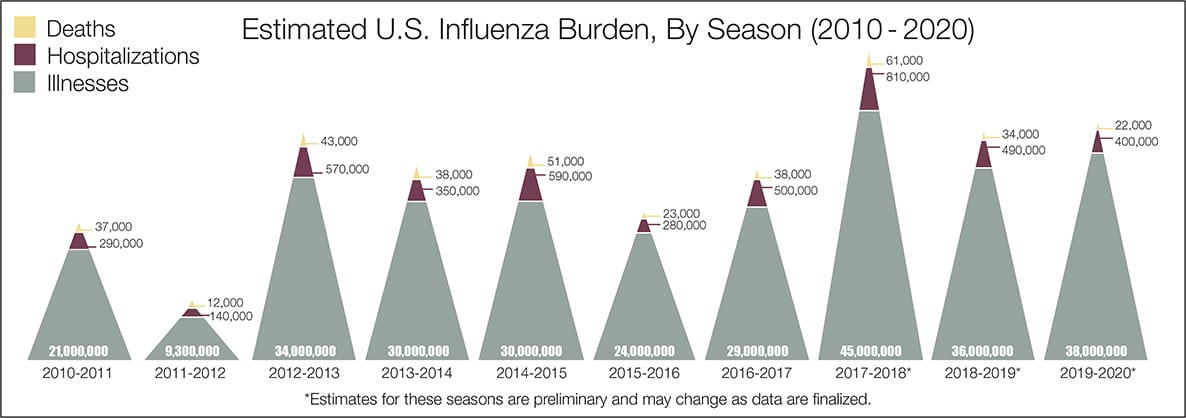
(To view the original image, which you can enlarge, go to https://www.cdc.gov/flu/images/about/burden/influenza-burden-chart2-960px.jpg)
2017-2018*
UNITED STATES ONLY (Numbers in parentheses are the low to high estimates)
45,000,000 (39,000,000 – 58,000,000) INFECTED/CONFIRMED
21,000,000 (18,000,000 – 27,000,000) MEDICAL VISITS
810,000 (620,000 – 1,400,000) HOSPITALIZATIONS
61,000 (46,000 – 95,000) DEATHS
CDC estimates that influenza has resulted in between 9 million – 45 million illnesses, between 140,000 – 810,000 hospitalizations, and between 12,000 – 61,000 deaths annually since 2010.
The 2019-2020 FLU season was still ongoing when COVID-19 APPEARED IN THE U.S. AND STATS WERE GIVEN WEEKLY THROUGH APRIL.
The image below was for the week ending August 1, 2020.
LET'S LOGICALLY ASK OURSELVES THIS:
"SINCE CDC DOES NOT REQUIRE AUTOPSY RESULTS TO PROVE/DISPROVE COVID-19 (CV-19) AS CAUSE OF DEATH, DOES NOT DISTINGUISH BY 100% PROOF BETWEEN PNEUMONIA DEATHS FROM FLU AND PNEUMONIA DEATHS FROM
CV-19, HOW MANY DEATHS ATTRIBUTED TO CV-19 ARE ACTUALLY DEATHS FROM THE CURRENT FLU?"
BELOW ARE THE STATS FOR 2019-2020 FLU SEASON, FLU, NOT COVID-19.

30% of Americans who were tested, had tested positive!
In fact, from week 52 (the last week of 2019) until week 9 of 2020, over 1/4th of those tested for influenza were testing positive.
Then, after the first case of CV-19 was found and announced in the U.S., on January 21, 2020, the flu almost completely disappeared.
'Miracle', manipulation of data, cessation of collecting flu data?
What happened?
CDC NOTE: The week of April 4 was the last week in-season influenza burden estimates will be provided for the 2019-2020 season. *Because influenza surveillance does not capture all cases of flu that occur in the U.S., CDC provides these estimated ranges to better reflect the larger burden of influenza.
WHAT ABOUT THIS...
"CORONAVIRUS CASES TESTED IN U.S. REMOVED FROM CDC WEBSITE, ACCORDING TO CONGRESSMAN: 'AMERICAN PEOPLE DESERVE ANSWERS.'
NEWSWEEK:
"This is unacceptable.I just sent a letter to @CDCDirector demanding answers to why their website removed public data on the number of patients tested in the United States. The American people deserve answers."
Here is another chart that clearly shows the DRAMATIC AND SUDDEN DECLINE IN FLU CASES ONCE WE HAD CV-19 IN AMERICA.

There was no GRADUAL decline from week 10 to week 14...IT DROPPED LIKE A ROCK.
Americans stopped getting the FLU and started getting....(drum-roll, please)...
COVID-19, 'THE KILLER VIRUS'.
AT THE PEAK OF THIS FLU SEASON, AMERICANS SUDDENLY STOPPED BEING TESTED FOR FLU???
Tests just suddenly stopped although 1/4th of those being tested were testing positive?
THAT MAKES NO LOGICAL (OR MEDICAL) SENSE AT ALL!
America was riddled with INFLUENZA, an estimated 45 MILLION cases.
Did those who were infected just suddenly STOP INFECTING OTHERS?
NOBODY WAS WEARING MASKS, NOBODY WAS SOCIAL-DISTANCING, FEW SCHOOLS HAD CLOSED, BUSINESSES WERE NOT SHUT DOWN AND IT WAS A NEW PEAK IN OUR FLU SEASON.
BUT THEN, IN JUST 3 WEEKS, BAM! NO MORE INFLUENZA???
FLU MORTALITY RATE PEAKED AT WEEK 10 OF 2020 (in March), WAS VERY HIGH, YET HAD PLUMMETED BY WEEK 20 AND DROPPED OFF TO ALMOST NONE BY WEEK 30 (BEGINNING OF AUGUST).
2019-2020 PEDIATRIC MORTALITY RATE RAN HIGH AND WE LOST 187 CHILDREN TO INFLUENZA AS OF TODAY; CHILDREN HAVE ALWAYS BEEN MORE AT RISK OF DYING FROM INFLUENZA THAN FROM CV-19.

BUT, AGAIN, SUDDENLY THAT RATE DRAMATICALLY DROPPED OFF AND WE SEE NO PEDIATRIC DEATHS LISTED AFTER WEEK 19 OF 2020 (MAY).
HOW AMAZING IS THAT?
PEDIATRIC DEATHS BY FLU ARE THE ONLY SOLID (NOT ESTIMATED) DATA COLLECTED EACH FLU SEASON. REPORTING PEDIATRIC DEATHS BY INFLUENZA IS MANDATORY.
CDC estimates* that, from October 1, 2019, through April 4, 2020, there have been:
-- 39,000,000 – 56,000,000 flu illnesses
-- 18,000,000 – 26,000,000 flu medical visits
-- 410,000 – 740,000 flu hospitalizations
-- 24,000 – 62,000 flu deaths
ABOUT THOSE HOSPITALIZATIONS...
THAT CHART ENDS ABRUPTLY AS DID THE OTHERS< JUST AS IT, TOO, WAS CLIMBING-- IN APRIL.
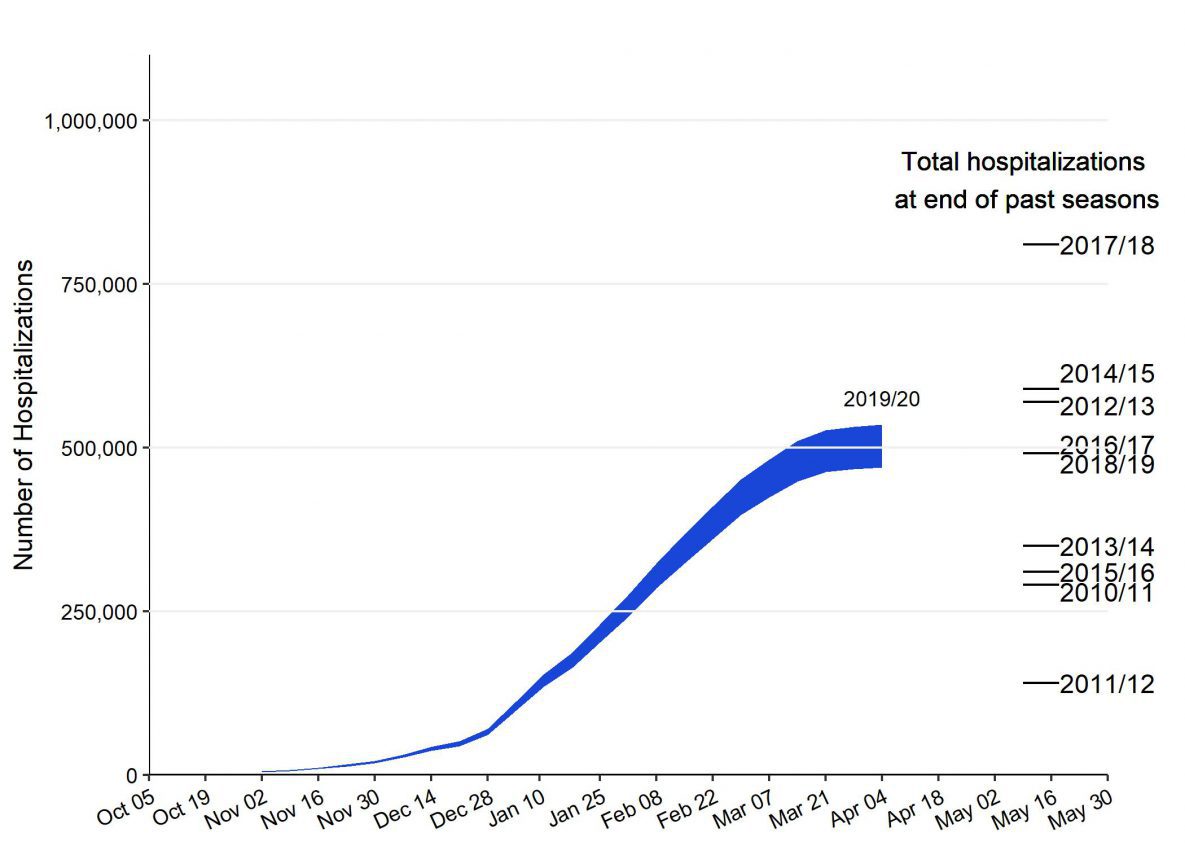
WHAT HAPPENED IN APRIL, 2020?
On April 2, Spain announced it had surpassed 10,000 deaths as its coronavirus crisis worsened.
On April 24, it was announced that various countries will test people-tracking wristbands to ensure people are staying home.(CNN/BBC)
According to the Johns Hopkins study, nearly 53,000 people have died from the new coronavirus WORLDWIDE.
BTW, how many of you are aware, through mainstream or social media, that about 20% of the COMMON COLD CASES ARE CORONAVIRUSES?
IN MARCH, 2020, MANY STATES STAY-AT-HOME ORDERS WENT INTO EFFECT. AND AMERICA BASICALLY WENT ON LOCK-DOWN FOR "NON-ESSENTIAL BUSINESSES", SCHOOLS, CHURCH-GATHERINGS, ETC.
SOCIAL GATHERING BUSINESSES LIKE RESTAURANTS, MOVIE THEATERS, BARS AND U.S. BEACHES WERE CLOSED.
The National Park System closed or limited the public’s access to a majority of park sites.
Social contacts were severely limited.
BUT WAIT, THERE ARE ALSO SERIOUS LIMITATIONS TO FLU DATA COLLECTION, MAKING THE CDC ESTIMATES TOO LOW.
Limitations
"The estimates of the cumulative burden of seasonal influenza are subject to several limitations.
First, the cumulative rate of laboratory-confirmed influenza-associated hospitalizations reported during the season may be an under-estimate of the rate at the end of the season because of identification and reporting delays.
Second, rates of laboratory-confirmed influenza-associated hospitalizations were adjusted for the frequency of influenza testing and the sensitivity of influenza diagnostic assays. However, data on testing practices during the 2019-2020 season are not available in real-time.
CDC used data on testing practices from the past influenza seasons as a proxy. Burden estimates will be updated at a later date when data on contemporary testing practices become available.
Third, estimates of influenza-associated illness and medical visits are based on data from prior seasons, which may not be accurate if the seriousness of illness or patterns of care-seeking have changed."
ALL CHARTS AND DATA ARE FROM CDC's OWN WEBSITE.
THERE IS ONE MORE PERTINENT BIT OF INFO YOU MAY HAVE MISSED IN ALL THE FEAR-MONGERING MAINSTREAM MEDIA HYPE ABOUT REPORTING CV-19 DEATHS.
LISTING A DEATH AS DEATH FROM/WITH COVID-19 REQUIRES NO MEDICAL PROOF, JUST A CHECK-BOX AND A SIGNATURE.
Causes of death are coded according to the International Classification of Diseases, 10th Revision (ICD–10).
On January 31, 2020, the World Health Organization (WHO) established a new emergency code for COVID-19: U07.1.
The WHO has provided a second code, U07.2, for clinical or epidemiological diagnosis of COVID-19 where a laboratory confirmation is inconclusive or not available.
Because laboratory test results are not typically reported on death certificates in the United States, NCHS did not implement U07.2 for mortality statistics.
IN CDC's OWN WORDS:
"This document provides specific guidance for the collection and submission of postmortem specimens from deceased known or suspected COVID-19 cases.
Medical examiners, coroners, and other healthcare professionals should use professional judgment to determine IF a decedent had signs and symptoms compatible with COVID-19 during life and whether postmortem testing is necessary.
"Autopsies on decedents known or suspected to be COVID-19 cases should be conducted in Airborne Infection Isolation Rooms (AIIRs).
These rooms:
--Are at negative pressure to surrounding areas
--Have a minimum of 6 air changes per hour (ACH) for existing structures and 12 ACH for renovated or new structures
--Have air exhausted directly outside or through a high efficiency particulate aerosol (HEPA) filter
Doors to the room should be kept closed except during entry and egress.
If an AIIR is not available, ensure the room is negative pressure with no air re-circulation to adjacent spaces.
A portable HEPA re-circulation unit could also be placed in the room to provide further air filtration."
AFTER ALL THAT, SPECIMENS MUST BE "FIXED", STORED AND SHIPPED PER CDC GUIDELINES.
THEN THE COLLECTING FACILITY MUST SUBMIT A REQUEST TO SEND THE SPECIMENS AND WAIT FOR APPROVAL.
IF APPROVED, CDC MAY STILL REJECT RECEIVED SPECIMENS THAT DO NOT MEET THEIR CRITERIA.
THERE IS A CDC-WRITTEN REPORTING GUIDELINE IN PDF FORM <HERE>.
IT'S WORTH THE READ JUST TO SEE HOW EASY IT IS TO REPORT ANY DEATH AS CV-19 RELATED.
IF ONE "SUSPECTS" A PERSON DIED OF/WITH CV-19, JUST CHECK THE BOX AND SIGN.
TESTING IS A KEY TO STOPPING CV-19 SPREAD BECAUSE IT IDENTIFIES THOSE WHO HAVE CV-!( BUT ARE WITHOUT SYMPTOMS.
CDC's PREFERRED COVID-19 "TESTING" IS A JOKE.
Intially, the CDC refused to use the tests already available that the World Health Organization offered. Other nations, even China, offered the CDC/USA test kits and they were refused.
CDC was maligned more than once by The Atlantic and other media for refusing those tests.
CDC dragged their feet and cost America time and perhaps many deaths because we weren't testing and then quarantining those who tested positive.
CDC 'invented' their own test kits, which had to be recalled.
The CDC lab in Atlanta was found to be contaminated... with CV-19.
It was like watching an old "Keystone Cops" movie, bungling error after error.
"This is not merely a technical error. States have set quantitative guidelines for reopening their economies based on these flawed data points."
“You’ve got to be kidding me,” Ashish Jha, the K. T. Li Professor of Global Health at Harvard and the director of the Harvard Global Health Institute, told us when we described what the CDC was doing. “How could the CDC make that mistake? This is a mess.”
Knowing full well the that SEROLOGICAL (BLOOD) TESTS are more trustworthy, give results more quickly than their swabbing, and have a lower FAILURE RATE than swabbing, CDC made sure that such tests were maligned in the U.S. mainstream media (MSM).
"Per FDA guidance, antibody tests have not been validated for diagnosis of COVID-19 infection, and antibody tests by themselves are of limited value in the immediate diagnosis of a patient where COVID-19 infection is suspected."
WELL, FDA CHANGED ITS MIND:April 18, 2020
Statement From:Commissioner of Food and Drugs - Food and Drug AdministrationStephen M. Hahn M.D. "As the country starts to see positive signs that the mitigation efforts, like stay-at-home orders and social distancing, are working in our fight against the COVID-19 pandemic, the question of when we can return to work and resume our normal activities is one of the most critical issues facing our nation.
Antibody tests – also known as serological tests – may have the potential to play a role in this complex calculation. Results from these tests can help identify who has been infected and developed antibodies that may protect from future infection as well as identify those still at risk. Results can also help inform who may qualify to donate blood that can be used to manufacture convalescent plasma, an investigational product for use with those who are seriously ill from COVID-19.
To date, we have already issued four EUAs for serological tests, and we expect that number to continue to grow in the coming weeks. The FDA encourages developers to submit EUA requests for their tests, as an EUA will provide laboratories and providers with assurance that FDA has reviewed that test.
The FDA issued a policy explaining that FDA does NOT intend to object when developers of serological tests market or use their tests without prior FDA review where: 1) the tests are validated by the developer to determine that they are accurate and reliable, 2) notification of the developer’s validation is provided to FDA, and 3) the tests are labeled appropriately."
MEANWHILE, CHINA AND OTHER NATIONS TURNED TO THE "GOLD STANDARD" IN RAPID TESTING, THE "REAL TIME RT-PCR" COMBINED WITH CHEST CT .FROM THE JOURNAL OF CLINICAL MICROBIOLOGY, Published: 4 March 2020.:
"Improved Molecular Diagnosis of COVID-19 by the Novel, Highly Sensitive and Specific COVID-19-RdRp/Hel Real-Time Reverse Transcription-PCR Assay Validated In Vitro and with Clinical Specimens"
HOWEVER, GOOD TESTING FOR CV-19 HAS BEEN HARD TO FIND.
"Laboratory Diagnosis of COVID-19: Current Issues and Challenges""This commentary addresses current issues for the laboratory diagnosis of COVID-19 that must be understood by clinicians, clinical microbiology laboratories, and public health authorities.
Other respiratory viral pathogens such as influenza and respiratory syncytial viruses must be ruled out.
There are a number of coronaviruses that cause respiratory and intestinal infections in humans.
Serological methods, when available, will play an important role in the epidemiology of COVID-19 and in determining the immune status of asymptomatic patients but are unlikely to play any role in screening or for the diagnosis of early infections."
Mayo Clinic doctors find many COVID-19 antibody tests fail ...
"By Feb. 25, Chu and her colleagues could not bear to wait any longer. They began performing coronavirus tests, without government approval.
What came back confirmed their worst fear. They quickly had a positive test from a local teenager with no recent travel history. The coronavirus had already established itself on U.S. soil without anybody realizing it."
WHAT IS THE BOTTOM LINE ON THIS CV-19 MADNESS?
THE CDC STALLED EARLY TESTING WHILE UNKNOWN CARRIERS OF THE VIRUS SPREAD IT THROUGHOUT AMERICA; THE TESTS ARE NOT ACCURATE ENOUGH; CDC DOESN'T WANT ANTIBODY TESTS (ESPECIALLY POSITIVE ONES) BECAUSE THAT WOULD FURTHER LOWER THE DEATH RATE (A DEATH RATE THAT IS COMPARABLE TO A HIGH-INFECTION SEASONAL FLU); CV-19 HAS BECOME A HIGHLY POLITICIZED CRAP-SHOOT THAT HAS RUINED THE ECONOMY OF ENTIRE NATIONS, CAUSED A SERIOUS RISE IN SUICIDES, HOMICIDES, DOMESTIC VIOLENCE AND DEPRESSION AND ANXIETY IN JUST ABOUT EVERY NATION ON EARTH, HEAVILY AIDED BY A BIASED NEWS MEDIA THAT IS USING FEAR-MONGERING TO MAKE THE WORLD'S POPULATION COMPLY WITH ALL MOSTLY USELESS MANDATES OF THIS NEW SCARE TACTIC OF A DAMNED VIRUS THAT IS SO "DEADLY" THAT WE HAVE TO TAKE A TEST TO KNOW WE HAVE OR HAD IT.
IT'S A 'ONE-TRICK PONY' SHOW.
"Dr." Faucci has stated that a vaccine would be maybe 50% effective, but it has been insinuated that we will HAVE to take the vaccine to travel freely, that it WILL BE MANDATORY.
FEMA has the absolute power to gather the non-compliant and quarantine them wherever FEMA pleases.
Someone out there in the "Ivory Tower" wants tracking included in the vaccine. Insertion of a microchip the size of a BB via hypodermic injection is already easy and the person thus injected would likely be unaware of the presence of the chip. “Having the chip inserted was a breeze, no real pain to report of.”
“Having the chip inserted was a breeze, no real pain to report of.”

SMALLER...
Hitachi “Powder”/”Dust” µ-Chip Ultra-Small Micro RFID Chip with Embedded Antenna for Military and (Clandestine) Intelligence/Surveillance Applications.

"Japanese electronics giant Hitachi has just developed a super-small 128-bit ROM (Read-Only Memory) micro RFID (Radio Frequency IDentification) chip that can store a 38-digit number and looks like a black grain of sand. It measures 0.15 x 0.15 millimeters across and 7.5 micrometers thick.
The Defense Department is developing a new, mood-predicting brain chip to treat PTSD in soldiers.MAY 28, 2014
{kind=link}
"With $12 million (and the potential for $26 million more if benchmarks are met), the Defense Advanced Research Projects Agency, or DARPA, wants to reach deep into your brain’s soft tissue to record, predict and possibly treat anxiety, depression and other maladies of mood and mind. Teams from the University of California at San Francisco, Lawrence Livermore National Lab and Medtronic will use the money to create a cybernetic implant with electrodes extending into the brain. The military hopes to have a prototype within 5 years and then plans to seek FDA approval."
AND THEY DID JUST THAT.
Oct. 23, 2019 — "BrainChip, a leading provider of ultra-low power, high performance edge AI technology, has been awarded a new patent for dynamic neural function libraries, a key component of its AI processing chip Akida.
United States Patent number 10,410,117 addresses a dynamic neural network within an AI device.
BrainChip’s intellectual portfolio consists of 11 patents issued or in process, including a foundational patent in the area of Spiking Neural Networks (SNN) that has been cited by leading companies such as IBM, Qualcomm, Samsung, and Hewlett Packard."
SO, LOOKING AT THE WHOLE THING, AS TESTING RAMPS UP, THERE IS SURE TO BE AT LEAST 5 THINGS WE CAN EXPECT TO SEE:
1--A SHARP RISE IN CV-19 INFECTIONS WITH SPIKES WHEREVER 'THEY' PLEASE BECAUSE THEY CONTROL THE RELEASE OF DATA AND HAVE ALSO SUSPENDED (???) TESTING FOR INFLUENZA.
HAVING THE FLU MAY BECOME, "YOU HAVE CV-19"?
2-- DEATH RATES WILL ALSO SPIKE BECAUSE CAUSE OF DEATH NO LONGER HAS TO BE PROVEN.
WE'VE SEEN EVIDENCE OF THAT <HERE>, <HERE> , as reported by NEWSWEEK, AND <HERE>, where data analyzed from 110 health care locations in Florida show everyone who went to them tested positive for COVID-19. but the labs all say the data was WRONG.
The death rate must keep pace with positive tests, and the serum antibody test will show millions more of us have already had and recovered from CV-19.
Those who have antibodies for the virus will NOT need a vaccine, you see.
They are now immune.
3-- THE VACCINE (probably chosen this Fall) WILL BE MANDATORY, likely for school-age children and the military first, then for the rest of us.
We can already see signs of mandatory, i.e. FORCED COMPLIANCE, of idiotic 'mandates' in instances like the two people fined $1000 each for not checking in with Connecticut's virus police after traveling to Florida and Louisiana.
AND THIS: "Maryland Gov. Larry Hogan says arrest for coronavirus offense sends 'great message'
He has a lot of company from other governors doing the same thing...UNCONSTITUTIONALLY, BTW.
4-- FOOD SHORTAGES "DUE TO COVID-19".
04/22/2020
"World Food Program Executive Director David Beasley told the U.N. Security Council that even before COVID-19 became an issue, he was telling world leaders that “2020 would be facing the worst humanitarian crisis since World War II.” That’s because of wars in Syria, Yemen and elsewhere, locust swarms in Africa, frequent natural disasters and economic crises including in Lebanon, Congo, Sudan and Ethiopia, he said.
“In a worst-case scenario, we could be looking at famine in about three dozen countries, and in fact, in 10 of these countries we already have more than one million people per country who are on the verge of starvation,” he said."
FROM BLOOMBERG, June 9, 2020:
"The coronavirus overturned the global food supply chain. With supermarket shelves stripped by panic buying, livestock destroyed because meat-packing plants had shut, and quarantined consumers battling to get deliveries, food security, self-sufficiency and urban farming suddenly became household words and governments started to reexamine how their countries are fed."
5-- CDC, FDA AND OTHERS WILL NOT RELENT ON THE LIFE-SAVING DRUG COMBINATION THAT CHINA, SPAIN, FRANCE, ITALY, SOUTH KOREA, ISRAEL, BRAZIL AND A FEW OTHERS HAVE USED ALMOST SINCE CV-19 BEGAN.
There are currently 925,297 CV-19 cases in ALL of Africa, where HFC is given freely to wide populations, including children and pregnant women, because malaria there is such a threat.
People worldwide have safely taken the HFC for 6 DECADES.
My previous blog, , showed the clinical efficacy of using the drug, and of using the drug combo, both as a treatment and a prophylactic.
MY THOUGHT IS THAT IF WE WERE ALLOWED FREE USE OF THE SAME DRUG(S), SAVED THOUSANDS OR EVEN MILLIONS OF LIVES, A MANDATORY VACCINE WOULD NOT BE SO EASY TO SELL TO A FEARFUL POPULACE.
Those who don't want to usse a proven drug combo certainly would NOT have to do so.
CAN THE SAME BE SAID FOR THOSE WHO DON'T WANT ANOTHER DAMNED VACCINE?
NO.
CAN AMERICANS CHOOSE TO TAKE HFC OR THE HFC-ZITHROMAX-ZINC COMBINATION IF THEY WANT IT?
NO.
SEEMS THAT THE MANTRA OF THE 'LEFT', "MY BODY, MY CHOICE!", NEVER APPLIES TO THE 'RIGHT'.
WRAPPING IT UP, HAVE A LOOK AT THIS QUESTION:
How can my lab get the COVID-19 virus?
"The National Institute of Health (NIH)’s Biodefense and Emerging Infections Research Resources Repositoryexternal icon (BEI Resources) will provide laboratories with COVID-19."
THOSE ARE THE GUYS WHO SEARCH THE WORLD FOR NEW, ANCIENT, DEADLIER VIRUSES THAN OUR ENEMIES MAY HAVE, FOR OUR, UMMM, "DEFENSE".
THIS IS FROM THE ABOVE-LINKED WEBSITE:
"Who Can Use This Resource?
Users, domestic or foreign, must be a principal investigator, laboratory director, or equivalent in a public or academic institution, or a director of research or equivalent in a private or for-profit institution
Users must work in an established institution with appropriate facilities and safety programs for the appropriate level of registration requested
Users need not be a grantee of NIAID or another National Institutes of Health Institute or Center
There is no charge for the materials (shipping and handling fees may apply).
THESE ARE THE SAME GUYS WHO GAVE SADDAM HUSSEIN BIOLOGICAL WEAPONS SAMPLES.
"A letter written in 1995 by former CDC Director David Satcher to former Senator Donald W. Riegle, Jr., points out that the U.S. Government provided nearly two dozen viral and bacterial samples to Iraqi scientists in 1985--samples that included the plague, botulism, and anthrax, among other deadly diseases.
U.S. LABS HAVE BEEN "STUDYING" CORONAVIRUSES FOR YEARS.
How secure are labs handling world's deadliest pathogens?
“As more of this kind of research occurs, and it will, especially internationally, the risks of both accidental release or potential theft and misuse will increase as well,” Salerno said. “The science is way ahead of governments’ ability to regulate the science.”
"Some scientists argue that the experiments creating contagious H5N1 mutants should be done only at BSL-4 facilities.
“An escape would still produce the worst pandemic in history,” said Michael Osterholm of the University of Minnesota..."
IS THERE A BSL-4 OR OTHER VIRUS LAB NEAR YOU?

AND ALSO, THE DEADLIEST KNOWN PLAGUE IN ALL THE WORLD, 'SEPTICEMIC PLAGUE", HAS JUST CLAIMED A VICTIM IN....NEW MEXICO.
HE WAS IN HIS 20s AND WAS THE SECOND PERSON REPORTED TO BE INFECTED THERE.
"Human Yersinia infections most commonly result from the bite of an infected flea or occasionally an infected mammal, but like most bacterial systemic diseases, the disease may be transmitted through an opening in the skin or by inhaling infectious droplets of moisture from sneezes or coughs."
Bubonic plague was diagnosed in a Santa Fe County, NM man in his 60s, the agency reported July 27.
MEANWHILE, FAR FROM WUHAN, Bubonic plague: Third case reported in China.
RELATED: Squirrel in Colorado Tests Positive for the Bubonic Plague
2020 HAS BEEN A HELLUVA YEAR.
___________________________
Addendum & End Notes:
--Dr. Kary Mullis invented the polymerase chain reaction (PCR) testing method in 1985 that is CDC's PREFERRED test method today.
Mullis was recognized for this achievement by being awarded the Nobel Prize in Chemistry in 1993.
Mullis died of pneumonia on August 7, 2019.
John Lauritsen, in December 1996, wrote, quoting Mullis,
--WHAT IS THE "GOLD STANDARD OF VIRUS TESTING?
THE REVERSE TRANSCRIPTION - POLYMERACE CHAIN REACTION (RT-PCR) TEST.
"As the coronavirus that causes the COVID-19 disease spreads across the world, the IAEA, in partnership with the Food and Agriculture Organization of the United Nations (FAO), is offering its support and expertise to help countries use real time reverse transcription–polymerase chain reaction (real time RT–PCR), one of the most accurate laboratory methods for detecting, tracking and studying the COVID-19 coronavirus.
But what is real time RT–PCR?
How does it work?
How is it different from PCR?
Real time RT–PCR is a nuclear-derived method for detecting the presence of specific genetic material in any pathogen, including a virus. Originally, the method used radioactive isotope markers to detect targeted genetic materials, but subsequent refining has led to the replacement of isotopic labelling with special markers, most frequently fluorescent dyes. This technique allows scientists to see the results almost immediately while the process is still ongoing, whereas conventional RT–PCR only provides results at the end of the process.
Real time RT–PCR is one of the most widely used laboratory methods for detecting the COVID-19 virus.
While many countries have used real time RT–PCR for diagnosing other diseases, such as Ebola virus and Zika virus, many need support in adapting this method for the COVID-19 virus, as well as in increasing their national testing capacities.
Some viruses such as the coronavirus (SARS-CoV-2), which causes COVID-19, only contain RNA, which means that they rely on infiltrating healthy cells to multiply and survive. Once inside the cell, the virus uses its own genetic code — RNA in the case of the COVID-19 virus — to take control of and ‘reprogramme’ the cells, turning them into virus-making factories.
In order for a virus like the COVID-19 virus to be detected early in the body using real time RT–PCR, scientists need to convert the RNA to DNA. This is a process called ‘reverse transcription’. They do this because only DNA can be copied — or amplified — which is a key part of the real time RT–PCR process for detecting viruses.
Scientists amplify a specific part of the transcribed viral DNA hundreds of thousands of times. Amplification is important so that, instead of trying to spot a minuscule amount of the virus among millions of strands of genetic information, scientists have a large enough quantity of the target sections of viral DNA to accurately confirm that the virus is present.
A sample is collected from the parts of the body where the COVID-19 virus gathers, such as a person’s nose or throat. The sample is treated with several chemical solutions that remove substances such as proteins and fats and that extract only the RNA present in the sample. This extracted RNA is a mix of the person’s own genetic material and, if present, the virus’s RNA.
The RNA is reverse transcribed to DNA using a specific enzyme. Scientists then add additional short fragments of DNA that are complementary to specific parts of the transcribed viral DNA. If the virus is present in a sample, these fragments attach themselves to target sections of the viral DNA. Some of the added genetic fragments are used for building DNA strands during amplification, while the others are used for building the DNA and adding marker labels to the strands, which are then used to detect the virus.
Why use real time RT–PCR?
The real time RT–PCR technique is highly sensitive and specific and can deliver a reliable diagnosis in as little as three hours, though laboratories take on average between six and eight hours.
Compared to other available virus isolation methods, real time RT–PCR is significantly faster and has a lower potential for contamination or errors, as the entire process can be carried out within a closed tube. It continues to be the most accurate method available for the detection of the COVID-19 virus.
However, real time RT–PCR cannot be used to detect past infections, which is important for understanding the development and spread of the virus, as viruses are only present in the body for a specific window of time. Other methods are necessary to detect, track and study past infections, particularly those which may have developed and spread without symptoms.
//WW
Those who have antibodies for the virus will NOT need a vaccine, you see.
They are now immune.
3-- THE VACCINE (probably chosen this Fall) WILL BE MANDATORY, likely for school-age children and the military first, then for the rest of us.
We can already see signs of mandatory, i.e. FORCED COMPLIANCE, of idiotic 'mandates' in instances like the two people fined $1000 each for not checking in with Connecticut's virus police after traveling to Florida and Louisiana.
AND THIS: "Maryland Gov. Larry Hogan says arrest for coronavirus offense sends 'great message'
He has a lot of company from other governors doing the same thing...UNCONSTITUTIONALLY, BTW.
4-- FOOD SHORTAGES "DUE TO COVID-19".
04/22/2020
"World Food Program Executive Director David Beasley told the U.N. Security Council that even before COVID-19 became an issue, he was telling world leaders that “2020 would be facing the worst humanitarian crisis since World War II.” That’s because of wars in Syria, Yemen and elsewhere, locust swarms in Africa, frequent natural disasters and economic crises including in Lebanon, Congo, Sudan and Ethiopia, he said.
“In a worst-case scenario, we could be looking at famine in about three dozen countries, and in fact, in 10 of these countries we already have more than one million people per country who are on the verge of starvation,” he said."
FROM BLOOMBERG, June 9, 2020:
"The coronavirus overturned the global food supply chain. With supermarket shelves stripped by panic buying, livestock destroyed because meat-packing plants had shut, and quarantined consumers battling to get deliveries, food security, self-sufficiency and urban farming suddenly became household words and governments started to reexamine how their countries are fed."
5-- CDC, FDA AND OTHERS WILL NOT RELENT ON THE LIFE-SAVING DRUG COMBINATION THAT CHINA, SPAIN, FRANCE, ITALY, SOUTH KOREA, ISRAEL, BRAZIL AND A FEW OTHERS HAVE USED ALMOST SINCE CV-19 BEGAN.
There are currently 925,297 CV-19 cases in ALL of Africa, where HFC is given freely to wide populations, including children and pregnant women, because malaria there is such a threat.
People worldwide have safely taken the HFC for 6 DECADES.
My previous blog, , showed the clinical efficacy of using the drug, and of using the drug combo, both as a treatment and a prophylactic.
MY THOUGHT IS THAT IF WE WERE ALLOWED FREE USE OF THE SAME DRUG(S), SAVED THOUSANDS OR EVEN MILLIONS OF LIVES, A MANDATORY VACCINE WOULD NOT BE SO EASY TO SELL TO A FEARFUL POPULACE.
Those who don't want to usse a proven drug combo certainly would NOT have to do so.
CAN THE SAME BE SAID FOR THOSE WHO DON'T WANT ANOTHER DAMNED VACCINE?
NO.
CAN AMERICANS CHOOSE TO TAKE HFC OR THE HFC-ZITHROMAX-ZINC COMBINATION IF THEY WANT IT?
NO.
SEEMS THAT THE MANTRA OF THE 'LEFT', "MY BODY, MY CHOICE!", NEVER APPLIES TO THE 'RIGHT'.
WRAPPING IT UP, HAVE A LOOK AT THIS QUESTION:
How can my lab get the COVID-19 virus?
"The National Institute of Health (NIH)’s Biodefense and Emerging Infections Research Resources Repositoryexternal icon (BEI Resources) will provide laboratories with COVID-19."
THOSE ARE THE GUYS WHO SEARCH THE WORLD FOR NEW, ANCIENT, DEADLIER VIRUSES THAN OUR ENEMIES MAY HAVE, FOR OUR, UMMM, "DEFENSE".
THIS IS FROM THE ABOVE-LINKED WEBSITE:
"Who Can Use This Resource?
Users, domestic or foreign, must be a principal investigator, laboratory director, or equivalent in a public or academic institution, or a director of research or equivalent in a private or for-profit institution
Users must work in an established institution with appropriate facilities and safety programs for the appropriate level of registration requested
Users need not be a grantee of NIAID or another National Institutes of Health Institute or Center
There is no charge for the materials (shipping and handling fees may apply).
THESE ARE THE SAME GUYS WHO GAVE SADDAM HUSSEIN BIOLOGICAL WEAPONS SAMPLES.
"A letter written in 1995 by former CDC Director David Satcher to former Senator Donald W. Riegle, Jr., points out that the U.S. Government provided nearly two dozen viral and bacterial samples to Iraqi scientists in 1985--samples that included the plague, botulism, and anthrax, among other deadly diseases.
U.S. LABS HAVE BEEN "STUDYING" CORONAVIRUSES FOR YEARS.
How secure are labs handling world's deadliest pathogens?
“As more of this kind of research occurs, and it will, especially internationally, the risks of both accidental release or potential theft and misuse will increase as well,” Salerno said. “The science is way ahead of governments’ ability to regulate the science.”
"Some scientists argue that the experiments creating contagious H5N1 mutants should be done only at BSL-4 facilities.
“An escape would still produce the worst pandemic in history,” said Michael Osterholm of the University of Minnesota..."
IS THERE A BSL-4 OR OTHER VIRUS LAB NEAR YOU?
AND ALSO, THE DEADLIEST KNOWN PLAGUE IN ALL THE WORLD, 'SEPTICEMIC PLAGUE", HAS JUST CLAIMED A VICTIM IN....NEW MEXICO.
HE WAS IN HIS 20s AND WAS THE SECOND PERSON REPORTED TO BE INFECTED THERE.
"Human Yersinia infections most commonly result from the bite of an infected flea or occasionally an infected mammal, but like most bacterial systemic diseases, the disease may be transmitted through an opening in the skin or by inhaling infectious droplets of moisture from sneezes or coughs."
Bubonic plague was diagnosed in a Santa Fe County, NM man in his 60s, the agency reported July 27.
MEANWHILE, FAR FROM WUHAN, Bubonic plague: Third case reported in China.
RELATED: Squirrel in Colorado Tests Positive for the Bubonic Plague
2020 HAS BEEN A HELLUVA YEAR.
___________________________
Addendum & End Notes:
--Dr. Kary Mullis invented the polymerase chain reaction (PCR) testing method in 1985 that is CDC's PREFERRED test method today.
Mullis was recognized for this achievement by being awarded the Nobel Prize in Chemistry in 1993.
Mullis died of pneumonia on August 7, 2019.
John Lauritsen, in December 1996, wrote, quoting Mullis,
"Kary Mullis, who won the Nobel Prize in Science for inventing the PCR, is thoroughly convinced that HIV is not the cause of "AIDS".
With regard to the viral load tests, which attempt to use PCR for counting viruses, Mullis has stated: "Quantitative PCR is an oxymoron."
PCR is intended to identify substances qualitatively, but by its very nature is unsuited for estimating numbers.
Although there is a common misimpression that the viral load tests actually count the number of viruses in the blood, these tests cannot detect free, infectious viruses at all; they can only detect proteins that are believed, in some cases wrongly, to be unique to HIV.
The tests can detect genetic sequences of viruses, but not viruses themselves.
What PCR does is to select a genetic sequence and then amplify it enormously. It can accomplish the equivalent of finding a needle in a haystack; it can amplify that needle into a haystack. Like an electronically amplified antenna, PCR greatly amplifies the signal, but it also greatly amplifies the noise.
Since the amplification is exponential, the slightest error in measurement, the slightest contamination, can result in errors of many orders of magnitude.
Since the amplification is exponential, the slightest error in measurement, the slightest contamination, can result in errors of many orders of magnitude.
To make an analogy: using the viral load tests to gauge viral activity would be like finding a few fingernail clippings; amplifying the fingernail clippings into a small mountain of fingernail clippings mixed in with other junk; and then having an "expert" come along and interpret the pile as representing a platoon of soldiers, fully armed and ready for battle.
In short, the viral load tests are a scam.
When molecular biologists Peter Duesberg and Harvey Bialy analyzed the 1995 Ho and Wei papers (Nature 373) that launched the whole viral load bandwagon, they found that estimates of free virus had been overestimated by several orders of magnitude.
In the Wei study, 100,000 so-called "plasma viral RNA" units really amounted to less than 2 infectious viruses per milliliter of plasma.
And in the Ho study, 10,000 "plasma virions" corresponded to less than one infectious virus.
Duesberg and Bialy concluded, "there is no evidence for infectious virus in Wei et al.'s and Ho et al.'s patients." (Duesberg 1996a)
When molecular biologists Peter Duesberg and Harvey Bialy analyzed the 1995 Ho and Wei papers (Nature 373) that launched the whole viral load bandwagon, they found that estimates of free virus had been overestimated by several orders of magnitude.
In the Wei study, 100,000 so-called "plasma viral RNA" units really amounted to less than 2 infectious viruses per milliliter of plasma.
And in the Ho study, 10,000 "plasma virions" corresponded to less than one infectious virus.
Duesberg and Bialy concluded, "there is no evidence for infectious virus in Wei et al.'s and Ho et al.'s patients." (Duesberg 1996a)
When Australian mathematician Mark Craddock analyzed the same reports by Ho and Wei, he found gross errors in mathematics and logic, and in exasperation posed the question:
"Just what exactly will it take to get the people doing HIV research to turn away from high tech, unproven methods, arcane speculations about molecular interactions etcetera etcetera and ask themselves "Do any of us have the faintest idea what we are doing?"
--WHAT IS THE "GOLD STANDARD OF VIRUS TESTING?
THE REVERSE TRANSCRIPTION - POLYMERACE CHAIN REACTION (RT-PCR) TEST.
"As the coronavirus that causes the COVID-19 disease spreads across the world, the IAEA, in partnership with the Food and Agriculture Organization of the United Nations (FAO), is offering its support and expertise to help countries use real time reverse transcription–polymerase chain reaction (real time RT–PCR), one of the most accurate laboratory methods for detecting, tracking and studying the COVID-19 coronavirus.
But what is real time RT–PCR?
How does it work?
How is it different from PCR?
Real time RT–PCR is a nuclear-derived method for detecting the presence of specific genetic material in any pathogen, including a virus. Originally, the method used radioactive isotope markers to detect targeted genetic materials, but subsequent refining has led to the replacement of isotopic labelling with special markers, most frequently fluorescent dyes. This technique allows scientists to see the results almost immediately while the process is still ongoing, whereas conventional RT–PCR only provides results at the end of the process.
Real time RT–PCR is one of the most widely used laboratory methods for detecting the COVID-19 virus.
While many countries have used real time RT–PCR for diagnosing other diseases, such as Ebola virus and Zika virus, many need support in adapting this method for the COVID-19 virus, as well as in increasing their national testing capacities.
Some viruses such as the coronavirus (SARS-CoV-2), which causes COVID-19, only contain RNA, which means that they rely on infiltrating healthy cells to multiply and survive. Once inside the cell, the virus uses its own genetic code — RNA in the case of the COVID-19 virus — to take control of and ‘reprogramme’ the cells, turning them into virus-making factories.
In order for a virus like the COVID-19 virus to be detected early in the body using real time RT–PCR, scientists need to convert the RNA to DNA. This is a process called ‘reverse transcription’. They do this because only DNA can be copied — or amplified — which is a key part of the real time RT–PCR process for detecting viruses.
Scientists amplify a specific part of the transcribed viral DNA hundreds of thousands of times. Amplification is important so that, instead of trying to spot a minuscule amount of the virus among millions of strands of genetic information, scientists have a large enough quantity of the target sections of viral DNA to accurately confirm that the virus is present.
A sample is collected from the parts of the body where the COVID-19 virus gathers, such as a person’s nose or throat. The sample is treated with several chemical solutions that remove substances such as proteins and fats and that extract only the RNA present in the sample. This extracted RNA is a mix of the person’s own genetic material and, if present, the virus’s RNA.
The RNA is reverse transcribed to DNA using a specific enzyme. Scientists then add additional short fragments of DNA that are complementary to specific parts of the transcribed viral DNA. If the virus is present in a sample, these fragments attach themselves to target sections of the viral DNA. Some of the added genetic fragments are used for building DNA strands during amplification, while the others are used for building the DNA and adding marker labels to the strands, which are then used to detect the virus.
Why use real time RT–PCR?
The real time RT–PCR technique is highly sensitive and specific and can deliver a reliable diagnosis in as little as three hours, though laboratories take on average between six and eight hours.
Compared to other available virus isolation methods, real time RT–PCR is significantly faster and has a lower potential for contamination or errors, as the entire process can be carried out within a closed tube. It continues to be the most accurate method available for the detection of the COVID-19 virus.
However, real time RT–PCR cannot be used to detect past infections, which is important for understanding the development and spread of the virus, as viruses are only present in the body for a specific window of time. Other methods are necessary to detect, track and study past infections, particularly those which may have developed and spread without symptoms.
//WW
No comments:
Post a Comment