'It is unclear why quality control did not detect this issue': Early CDC tests couldn't distinguish between the coronavirus and water.
The CDC botched its early development of coronavirus test kits, which could not differentiate between the novel coronavirus and lab-grade water, according to a government email obtained by The Wall Street Journal."
AS OF TODAY, APRIL 18, 2020, WHO REPORTS 2,164,111 CONFIRMED CASES IN A WORLD OF ALMOST 8 BILLION PEOPLE.
WHO REPORTS 146,198 DEATHS, WORLDWIDE (COMPARED TO 80,000 DEATHS FROM INFLUENZA IN THE U.S. ALONE IN 2017-2018).
WHO REPORTS 665,330 CASES IN THE U.S. AND 30,384 DEATHS HERE, FEWER CASES BY MILLIONS AND FEWER DEATHS THAN WE'VE HAD SO FAR THIS SEASON FROM INFLUENZA, AND OUR FLU SEASON IS STILL ONGOING.
Doctors, congressmen, other medical professionals are starting to speak out with the truth about COVID-19.
When the WHO/CDC directed physicians to count ALL/ANY deaths as COVID-19 deaths as long as the deceased had a positive test for the new virus, several in the medical community finally began to rebel.
They know that this skews the numbers to a false high.
A patient admitted in end-stage renal failure, or in final days of terminal cancer, or with a massive coronary who tests positive for the new coronavirus is ruled a death BY Covid-19, not WITH, but BY.
This is false, the data is designed to keep the fear alive, the economy tanking, the obedience of the masses assured as people begin to realize that our normal flu season, every year, infects millions, sends hundreds of thousands to hospital, kills more Americans and certainly more worldwide than the new virus has, to date, AND THAT INFLUENZA KILLS MANY MORE CHILDREN THAT COVID-19.
And, unlike the new virus, the flu kills children by the hundreds during seasonal flu outbreaks.
ABOVE: Montana physician Dr. Annie Bukacek discusses how COVID 19 death certificates are being manipulated.“Stephen Schwartz, national director of the division of vital statistics, says in answer to the question as stated in the organization’s COVID-19 alert, “Should COVID-19 be reported on the death certificate only with a confirmed test?”
Check out his answer,
“COVID-19 should be reported on the death certificate for ALL decedents where the disease caused or is ASSUMED to have caused or CONTRIBUTED to death. Certifiers should include as much detail as possible based on their knowledge of the case, medical records, laboratory testing, etc.” …
“If a patient is positive for COVID-19 and dies from another cause such as pneumococcal sepsis, it may be considered accurate to say that person died with COVID-19 not from COVID-19. Yet the CDC guideline lists this case as one more COVID-19 death and they go to the next questionable death, they label that as COVID-19 and it goes on and on. You could see how these statistics have been made to look scary when it is so easy to add false numbers to the official database. Those false numbers are sanctioned by the CDC as of their memo yesterday, April 4th. …”
“The real number of COVID-19 deaths are not what most people are told and what they then think. How many people actually died from COVID-19 is anyone’s guess. …”
“Based on inaccurate, incomplete data, people are being terrorized by fear-mongers into relinquishing freedoms.” -Dr. Annie Bukacek
ABOVE: A STATE SENATOR AND ALSO A PHYSICIAN FROM MINNESOTA, SCOTT JENSEN COULD NOT ALLOW THE NEW MANDATE FOR REPORTING COVID-19 DEATHS TO GO UNCHALLENGED.
He rejected the conclusions being drawn by far right voices that over-hyping the COVID-19 crisis is a plot to destroy the reelection chances of President Donald Trump. “In medicine we don’t think that way,” he said.
On a previous television appearance on “Point of View” with Chris Berg, a local Fargo, N.D. news and opinion program, Jensen sketched a darker hypothesis.
When Berg asked Jensen why health officials would “skew” death figures, he responded.
“Well, fear is a great way to control people.” Asked to elaborate, he told the Reformer, “The fear with COVID-19 has been ratcheted unbelievably high. There have been a lot of figures in government who are trying to frighten people and, in that way, get them to do what they want.”
STANFORD DOCTORS ARE ALSO WARNING THAT THE DATA IS INSUFFICIENT.Dr. John Ioannidis of Stanford University explained why the estimates of COVID-19's death rate may be too high.
Ioannidis lifts the lid on our worrying lack of reliable data.
"We have gone into a complete panic state", says Dr. Ioannidis, describing the perfect storm that led Italy into crisis. The esteemed professor believes an exaggeration of the virus' mortality rate could lead the world to a fatal scenario: a lockdown lasting up to 18 months. "Then it is not just millions of lives at stake SARS-CoV-2, but billions, if we have to protract that for so long".
"We're likely overreacting to COVID and dooming ourselves to a horrible future."
Read his thoughts in writing here: https://www.statnews.com/2020/03/17/a...
Go here for the full-length interview with Dr John: https://youtu.be/d6MZy-2fcBw
Dr. Jay Bhattacharya is a professor of medicine at Stanford University. He is a research associate at the National Bureau of Economic Research and a senior fellow at both the Stanford Institute for Economic Policy Research and the Stanford Freeman Spogli Institute.
His March 24, 2020, article in the Wall Street Journal questions the premise that “coronavirus would kill millions without shelter-in-place orders and quarantines.”
In the article he suggests that “there’s little evidence to confirm that premise—and projections of the death toll could plausibly be orders of magnitude too high.”
In this edition of Uncommon Knowledge with Peter Robinson we asked Dr. Bhattacharya to defend that statement and describe to us how he arrived at this conclusion.
We get into the details of his research, which used data collected from hotspots around the world and his background as a doctor, a medical researcher, and an economist.
It’s not popular right now to question conventional wisdom on sheltering in place, but Dr. Bhattacharya makes a strong case for challenging it, based in economics and science.
"The northeastern Italian town of Vò, near the provincial capital of Padua. On March 6, all 3,300 people of Vò were tested, and 90 were positive, a prevalence of 2.7%.
Applying that prevalence to the whole province (population 955,000), which had 198 reported cases, suggests there were actually 26,000 infections at that time. That’s more than 130-fold the number of actual reported cases. Since Italy’s case fatality rate of 8% is estimated using the confirmed cases, the real fatality rate could in fact be closer to 0.06%."
By March, doctors reported that they still hadn't received enough tests to diagnose potential cases.
Matthew McCarthy, a hospitalist at Weill Cornell Medicine in New York City, told CNBC on March 2 that the revised CDC tests hadn't arrived at his hospital.
"I'm here to tell you right now — at one of the busiest hospitals in the country, I don't have it at my fingertips," he said. "I still have to call the Department of Health. I still have to make my case, plead, to test people."
March 31, 2020
WASHINGTON, D.C. – Today, U.S. Senator Rick Scott released the below statement calling on Congress to hold a hearing and investigate the World Health Organization’s (WHO) role in helping Communist China cover up information regarding the threat of the Coronavirus. In February, Senator Scott called on the WHO to do its own in-depth analysis on the extent of the Coronavirus – which they haven’t done. Senator Scott is gravely concerned about China’s efforts to isolate Taiwan when it comes global health and the WHO’s continued refusal to include Taiwan in its membership, meetings, and information, especially in the face of the Coronavirus. Senator Scott has also cosponsored legislation to increase the United States’ support of Taiwan’s efforts to join the WHO.
Senator Scott said, “The mission of the WHO is to get public health information to the world so every country can make the best decisions to keep their citizens safe. When it comes to Coronavirus, the WHO failed. They need to be held accountable for their role in promoting misinformation and helping Communist China cover up a global pandemic.
CALLING AN APPLE AN ORANGE.. WASHINGTON/NEW YORK (Reuters) - New York City, the hardest hit U.S. city in the coronavirus pandemic, revised its official COVID-19 death toll sharply higher to more than 10,000 on Tuesday, to include victims presumed to have perished from the lung disease but never tested.
"...VICTIMS" (????)...OF WHAT?
THE FLU?
PRE-EXISTING CONDITIONS?
STROKE OR HEART ATTACK?
ACCIDENTAL DEATHS?
VICTIMS OF WHAT?
THEY WERE NEVER TESTED FOR COVID-19 BY EITHER CDC's INACCURATE SWAB TESTS OR BY AUTOPSY!
The city’s revised count, 10,367 in all, raised the number of coronavirus deaths nationwide to more than 28,300.
"New York City’s Health Department said it will now also count ANY fatality deemed a 'PROBABLE' coronavirus death, defined as a victim whose death certificate lists as a cause of death ‘COVID-19’ or an equivalent.”
THIS IS BEING DONE SIMPLY TO DRIVE NUMBERS UP AND KEEP THAT FEAR FACTOR RAGING.
“There have been blunders, and there could be an underlying catastrophe that we don’t know about,” says epidemiologist Michael Mina, who helps run a microbiology testing lab at Brigham and Women’s Hospital. “It’s been very complicated and confusing for everyone with almost no clarity being provided by the CDC. There’s no good explanation for what’s going on here.”
The U.S. CDC decided to make its own coronavirus test, but the process was plagued by errors and delays. Here's a timeline of what went wrong.
-- The US is significantly behind on testing coronavirus patients compared to countries like South Korea and China.
-- Delays in US testing can be attributed, in part, to the CDC's decision to develop its own test, which turned out to be faulty.
-- The US also restricted testing criteria so that not everyone with symptoms of the virus was eligible to be tested.
-- The US response to the coronavirus outbreak has been plagued by testing debacles and delayed reports of local cases.
-- Around 80% of coronavirus cases are believed to be mild, and some patients may never show symptoms.
-- In states with major outbreak like Washington and New York, local hospitals have reported a shortage of test kits to identify cases. As of March 8, the CDC had only conducted around 1,700 tests, compared to nearly 200,000 in South Korea.
-- On February 6, WHO reported that it was shipping about 250,000 tests to 159 laboratories around the world.
CDC DECLINED THE TESTS!
The CDC shipped just 90 test kits to state public health labs on February 6 and 7.
90.A problem with one ingredient in the US tests caused more than half of state labs to receive inconclusive results.
William Schaffner, a CDC adviser and infectious-disease specialist at the Vanderbilt University School of Medicine, told Business Insider:
"The notion of accepting a test developed by someone else I think was a bit alien," Schaffner said. "There may have been other considerations of which I'm not aware, but I'm sure that pride was one of them: 'We know how to do this, thank you very much. We'll develop our own.'"
By the end of February, only three of the nation's more than 100 public-health labs had verified the CDC test for use.
"At first, CDC was the only place where testing could be performed," Richard Martinello, an associate professor of infectious disease at the Yale School of Medicine, told Business Insider. "For a country of our size, when you only have a single site doing that, it limits the resources available for testing."
Health experts said the CDC glitch was unprecedented.
"It ought to be foolproof. As a friend of mine said, it ought to be a gorilla test — even a gorilla can run it," CDC's own adviser and infectious-disease specialist William Schaffner said.
CDC WILL NOT DO A BETTER TEST, A BLOOD TEST.
WHY NOT?
Meanwhile, China developed a blood test that looked for specific antibodies produced by the body to fend off the virus.
The test worked even for patients in recovery, whereas PCR tests (the kind developed in the US) can only diagnose patients when they're ill.
Christian Drosten, a researcher at the German Center for Infection Research who developed one of the first COVID-19 tests, told Business Insider that it's helpful for countries to develop multiple tests in case one laboratory test turns out to be faulty.
"If we are in doubt about our test, or if there is something wrong with the test targets, the virus mutates or something, we could still switch to the test that another lab uses," Drosten said. "These are all in the public domain, and it's quite easy to switch."
WHY DIDN'T, WHY WON'T THE CDC SWITCH?
TOO FEW POSITIVES?
AS TESTING EXPANDS, THEY NEED DEATHS TO INCREASE OR ELSE PEOPLE MAY SEE THAT COVID-19 HAS FEWER CASES, HOSPITALIZATIONS AND DEATHS THAN OUR NORMAL FLU SEASON AND STOP LIVING IN TERROR.
The CDC's initial criteria called for testing only symptomatic patients with a travel history to China or those who may have had contact with a lab-confirmed coronavirus patient.
That meant the country's first case involving community spread, a patient in California, went untested for multiple days at two hospitals.
The CDC eventually revised its criteria on February 27 to include patients with conditions so severe that they required hospitalization. But some patients with mild symptoms, including those who recently traveled to countries with high case totals like Italy or Iran, still may not get tested right away.
BECAUSE THE MORE WHO TEST POSITIVE BUT DO NOT DIE FROM THE NEW VIRUS, THE BETTER THINGS LOOK AND THE LESS LIKELY PEOPLE ARE TO PANIC AND AGREE TO LOCKDOWNS, JOB LOSSES, A CRASHING ECONOMY?
The FDA began allowing academic hospital labs to develop and use their own coronavirus tests on February 29.
CDC REFUSED TO REPORT THESE TEST RESULTS ON THE CDC WEBSITE, BECAUSE CDC SAID THE FDA-APPROVED TESTS WERE 'UNVERIFIABLE'.
IMAGINE THAT!
THIS, AFTER THEIR OWN TESTS WERE KNOWN TO BE AND ADMITTED TO BE FAULTY AND AFTER THEIR OWN LAB IN ATLANTA WAS FOUND TO BE CONTAMINATED WITH COVID-19, MAKING FALSE POSITIVES LIKELY.U.S. coronavirus testing stalled for six weeks.
A SMALL GERMAN LAB MADE 1.4 MILLION TESTS DURING THAT TIME!
HOW CONVENIENT FOR CDC, RIGHT?
IN A NATION OF 340 MILLION PEOPLE, 665,330 AMERICANS HAVE TESTED POSITIVE FOR THE NEW VIRUS AND 30,384 HAVE DIED, BUT MAYBE NOT FROM THE VIRUS ITSELF. .
TO DIE STRICTLY BECAUSE OF COVID-19 IS DIFFERENT THAN DYING WITH MERELY A POSITIVE TEST FOR THE DISEASE.
THIS PAST FLU SEASON, CDC 'ESTIMATED' 60 MILLION INFLUENZA CASES, OVER 400,000 HOSPITALIZATIONS, 24,000 TO 62,000 DEATHS, INCLUDING ALMOST 170 CHILDREN.
IN 2017-2018, A RECORD 80,000 AMERICANS DIES OF FLU.
WE'RE STILL SEEING DEATHS FROM INFLUENZA AS FLU IS STILL MOSTLY "MODERATE TO WIDESPREAD" ACROSS MOST OF AMERICA.
MEANWHILE, WE'RE ALLOWING THE 'GOVERNMENT', STATE AND FEDERAL, TO DO THINGS THAT WE NEVER IMAGINED TO ALLOW BEFORE...GIVING UP MORE AND MORE OF OUR CONSTITUTIONAL RIGHTS EACH DAY, LIKE MINDLESS UNQUESTIONING SHEEP, WILLINGLY BECOMING PRISONERS OF FEAR.
Greg. G Wolff, an Epidemiologist with the Armed Forces Health Surveillance Branch recently published a study in the Journal Vaccine titled, "Influenza vaccination and respiratory virus interference among Department of Defense personnel during the 2017–2018 influenza season".
The study examined virus interference in a Department of Defense population, this refers to the increased risk of other respiratory viruses as a result of, in this case, the influenza vaccine.
The study found that virus interference varied among vaccinated individuals for individual respiratory viruses, and found that for coronavirus in particular, in this study, those who had been vaccinated with the flu vaccine had a 36 percent higher risk of contracting it
The study compared the vaccination status of more than two thousand people with non-influenza respiratory viruses to more than three thousand people with pan-negative results. The vaccination status of more than three thousand cases of influenza were compared to three different control groups, and appropriate adjustments were made.
The study points out that recently published studies have “described the phenomenon of vaccine-associated virus interference; that is, vaccinated individuals may be at increased risk for other respiratory viruses because they do not receive the non-specific immunity associated with natural infection.” It goes on to emphasize that
“There has been limited evidence that the influenza vaccine may actually be associated with the virus interference process. Other studies have found no association between influenza vaccination and increased respiratory virus risk.”
MEANWHILE, THE GOVERNMENTS AROUND THE WORLD ARE IMPSING TIGHTER AND TIGHTER REGULATIONS ON ALL OF US.
There's a video of Dr. Mike Ryan, the WHO's Emergencies Program director, saying that they: "May have to enter homes and remove family members."
WOULD YOU ALLOW THEM TO REMOVE YOUR CHILDREN, SPOUSE?
THEY REMOVED THE 4-YEAR-OLD DAUGHTER FROM THE HOME OF AN EMERGENCY ROOM DOCTOR IN FLORIDA, SIMPLY BECAUSE THE WOMAN WAS TREATING COVID-19 PATIENTS?
THAT'S LIKE THE OHIO NURSE, A SINGLE MOM WHO CAN'T AFFORD TO FIGHT IN COURT TO GET HER DAUGHTER BACK?
Tiffany DeMarcus, a nurse in Ohio, says the father of her child won’t return their young daughter because Tiffany is a nurse and has been exposed to COVID-19, WDTN reported.
LIKE THE CALIFORNIA DOCTOR MOM WHO'S LOST TWO DAUGHTERS BECAUSE SHE'S A DOCTOR TREATING COVID-19 PATIENTS?
Lisa Henning Low, an emergency room doctor in California, went to pick up her 7- and 10-year-old daughters from her ex-husband and ended up calling police after she says he pulled a gun and refused to let her take her children, KTVU reported.
When police arrived, her husband told officers he was worried Low was infecting their daughters because of her job in an emergency room, KTVU reported.
In Franklin County, Ohio, Domestic Court Judge Dana Preisse said parents have to have a court order to deviate from agreements, WDTN reported.
“You are to follow whatever shared parenting or custody plan that you have until there is another court order and to punish these folks because they are saving lives and are out there on the front line, you know, it’s just not right,” she told the outlet.
Brian Putnam, a family law attorney in Oklahoma City, said it’s hard to wrap his mind around working in the medical field being a legitimate reason to remove a parent’s children, KFOR reported.
“Oklahoma has an enormous medical community so if you play that out to its logical conclusion, everybody in the medical field would be at risk of losing their kids in a custody battle just because they work in a medical facility,” Putnam told the outlet.
In the disturbing video, Dr. Mike Ryan, the head of the World Health Organization's Emergencies Program, describes the W.H.O's egregiously invasive recommendation that health authorities may come into people's homes and take those suspected to be infected by COVID-19 to be quarantined, tested and presumably medicated against their will.
Clearly what the W.H.O. is proposing, modeled after China's approach, is a violation of basic civil and human rights.While this sounds outrageous and like a bad science fiction film, it is even more outrageous that hundreds of millions of people around the world are standing down in full compliance with whatever the authorities say should happen next.
The reality is that blind faith and compliance with the WHO's and CDC's "plan-demic" may very well result in the nightmarish scenario described by Dr. Ryan above.
The "frog" is already boiling.
Social distancing has already been unquestionably accepted the world over despite a significant body of evidence showing it can do great harm: 13 Studies Reveal How Social Distancing (i.e. Social Isolation) Can Increase Mortality. The reality is that independent epidemiological research on social distancing effectively reducing contagion-based morbidity and mortality is equivocal at best.
But the heat is slowly being turned up. A practice now being mandated in cities around the United States (and world), is the wearing of face masks.
The report FACE IT: The Evidence Proving the Effectiveness of Community Mask Wearing Doesn't Exist; The WHO Agrees sheds light on the reality that the WHO itself warns against the practice because it can make the problem worse. And so, if the practice does not prove "live saving" results as widely claimed, then it is more accurate to view it as an almost cult-like fetish or muzzle, demonstrating to the world one's unquestioning compliance in a form of full spectrum dominance this world has never before seen.
If we continue to give up our rights (even shaming or threatening those around us who don't comply), without question, it is unlikely there will be resistance when other agendas are unleashed, such as a Chinese-style social credit system is rolled out, mandatory vaccination, a digital ID tied to vaccination status, a 5G enabled real time surveillance network, a global governance system that will preempt the rights of individual nations, and many others.
All, ostensibly, to "save us from a virus," which truth be told, relative to the deaths from equally preventable causes such as heart disease, diabetes, and cancer, and even seasonal flu, makes a cruel mockery of the actions taken thus far in the name of saving us from COVID."
CDC ESTIMATES AN EXPECTED YEARLY DEATH TOLL OF 34,000 TO 67,000 HAVE DIED AND WILL DIE DURING EACH YEAR'S FLU SEASON JUST IN THE U.S., IN THE U.S.'s NORMAL FLU SEASON.
GO LOOK AT THE DAILY UPDATE FOR APRIL 18, 2020.
LOOK AT THE POORER NATIONS OF SOUTHEAST ASIA.
LOOK AT THE OIL RICH NATIONS OF THE MIDDLE EAST.
LOOK HOW FEW ARE "INFECTED" IN HEAVILY POPULATED INDIA, BANGLADESH AND AFRICA.
LOOK AT CANADA, MEXICO, THE SOUTH AMERICAN NATIONS.
JUST LOOK.
THE NUMBERS DO NOT SHOW THAT THIS IS "ANOTHER SPANISH FLU".
FROM THE GUARDIAN, UK: "We’ve been here before, and the direst predictions have not come to pass.""He stood behind a crested lectern, flanked by two scientists like five-star generals. He declared a four-point emergency strategy, plus 27 pages of “sweeping new powers” to meet “a national challenge”. He would call up retired health workers and army units. It was his first dry run at war.
The prime minister’s attempt to inspire calm was ridiculous. If calm was needed, why was he there? Within hours, the stock market plunged. Hundreds of flights were cancelled, even to places untouched by the virus. Workers were told to stay at home. Holiday bookings collapsed. Even James Bond was ordered to take fright and scurry home.
When hysteria is rife, we might try some history. In 1997 we were told that bird flu could kill millions worldwide. Thankfully, it did not. In 1999 European Union scientists warned that BSE “could kill 500,000 people”. In total, 177 Britons died of vCJD.
The first Sars outbreak of 2003 was reported by as having “a 25% chance of killings tens of millions” and being “worse than Aids”. In 2006, another bout of bird flu was declared “the first pandemic of the 21st century”, the scares in 2003, 2004 and 2005 having failed to meet their body counts.
Then, in 2009, pigs replaced birds. The BBC announced that swine flu “could really explode”. The chief medical officer, Liam Donaldson, declared that “65,000 could die”.
He spent £560m on a Tamiflu and Relenza stockpile, which soon deteriorated. The Council of Europe’s health committee chairman described the hyping of the 2009 pandemic as “one of the great medical scandals of the century”.
These scenarios could have all come to pass of course – but they represent the direr end of the scale of predictions. Should public life really be conducted on a worst-case basis?
Both Hancock and Britain’s chief medical officer, Chris Whitty, have struggled to contain the alarm. The government’s action plan pointed out that the virus is highly contagious, but the “great majority” of those who develop symptoms will experience only a “mild-to-moderate but self-limiting illness”. Every medical expert I have heard on the subject is reasonable and calm.
Not so politicians and the media. They love playing to the gallery, as they do after every health scare and terrorist incident. Front pages are outrageous. No BBC presenter seems able to avoid the subject. Wash hands to save the nation. The BBC must be sponsored by the soap industry.
It is always hard to reflect balance and perspective in news. In this case, it is surely essential. It would help if Hancock was handed back the virus brief by Downing Street.
It would also help if events were not cancelled, factories and offices not closed, and holidays not abandoned.
Of course, I could be wrong. I could get ill. Millions could die. But it is also possible that come the spring, this crisis will have passed. So for the moment, if you see a virus story containing “might” “could” “possibly” or “worst-case scenario”, stop reading. You are being fed war talk. Let them wash your hands, but not your brain.
• Simon Jenkins is a Guardian columnist
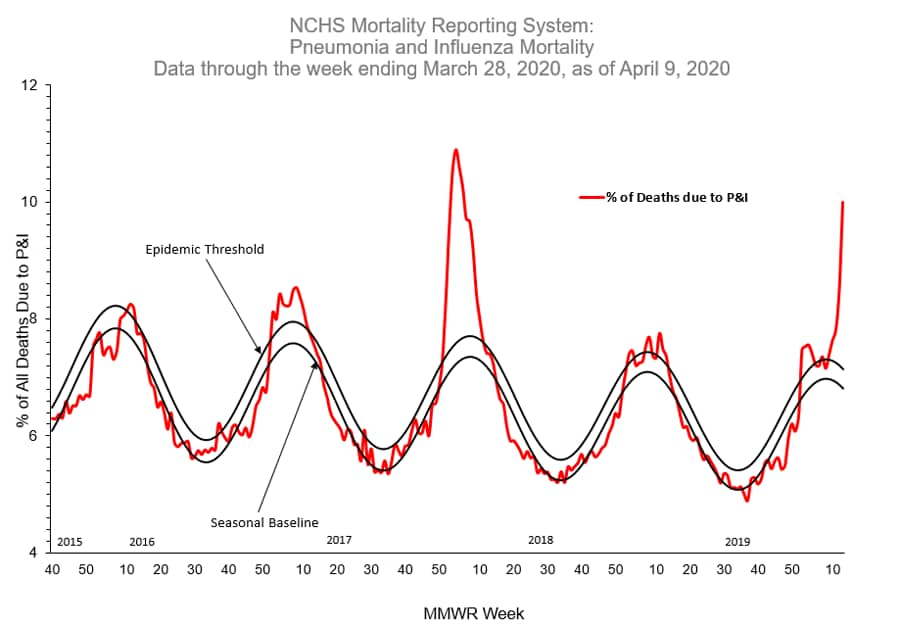
"Elevated influenza-like-illness is likely related to COVID-19."
"LIKELY"???
WHAT KIND OF SCIENCE OR STATISTICS IS "LIKELY"?
THEY'RE GRASPING AT EVERY STRAW TO FORCE THIS THING TO SPANISH FLU LEVELS.
BECAUSE THEY INTEND TO FORCE A VACCINE, A TERRIBLE, NIGHTMARISH VACCINE, THE LIKES OF WHICH THE WORLD HAS NEVER SEEN
WHAT ABOUT ALL THE OTHER YEARS, THE MANY RECENT YEARS THAT "significantly more P&I deaths occurred than would be expected at that time of year"?
THERE WAS NO COVID-19 TO BLAME THOSE DEATHS ON UNTIL JANUARY, 2020.
IT WASN'T SARS-CoV2 IN LATE 2019, IN 2018, IN 2017 WHEN WE HAD A REALLY BAD FLU SEASON, IN 2004-2005.
THEY'RE SO OBVIOUSLY USING FLU DEATHS TO UP THE NUMBERS FOR COVID-19 DEATHS..
THEY CREATED A PANIC LIKE THEY DID IN 2009-2010 ABOUT SWINE FLU, NAMED A(H1N1)pdm09, WHICH THEY BLAMED MANY DEATHS ON THEN, BUT THEY'VE DOWNPLAYED SWINE FLU EVER SINCE.
WHY?
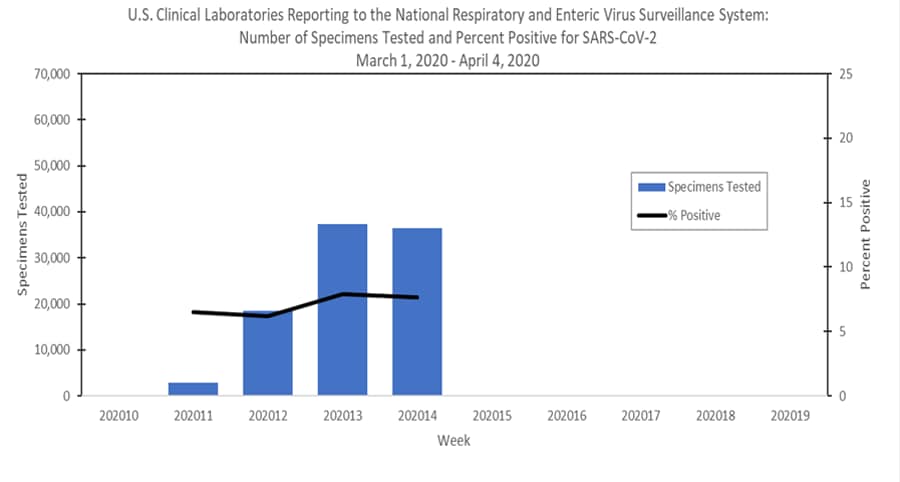
"CDC antigenically characterized 547 influenza viruses collected in the United States from September 29, 2019, to April 4, 2020.
We have observed an increase in the proportion of H1N1pdm09 viruses with this change late in the US season."
(THEY IDENTIFIED 212 OUT OF THE MEAGER TOTAL OF 547 SAMPLES, 547 FROM ALL AMERICA FOR AN ENTIRE FLU SEASON, UP TO APRIL 4.
DID HOSPITALS, HEALTH DEPARTMENTS, PRIVATE PRACTICES ALL STOP TESTING FOR FLU N APRIL 4th?
LOOKING AT THE CDC 'DIRECTIVE', THEY MAY HAVE!
86 A(H3N2) viruses were antigenically characterized by FRA with ferret antisera, and 40 (46.5%) were antigenically similar to cell-propagated A/Kansas/14/2017-like reference viruses representing the A(H3N2) component for the 2019-20 Northern Hemisphere influenza vaccines.
Influenza B Viruses
- B/Victoria: 201 B/Victoria lineage viruses, including viruses from both co-circulating sub-clades, were antigenically characterized by HI with ferret antisera, and 120 (59.7%) were antigenically similar to cell-propagated B/Colorado/06/2017-like reference viruses representing the B/Victoria component for the 2019-20 Northern Hemisphere influenza vaccines.
- B/Yamagata: 48 B/Yamagata lineage viruses were antigenically characterized by HI with ferret antisera, and all 48 (100%) were antigenically similar to cell-propagated B/Phuket/3073/2013-like reference viruses representing the B/Yamagata component for the 2019-20 Northern Hemisphere influenza vaccines.
A total of 556 additional viruses (211 A(H1N1)pdm09, 32 A(H3N2), and 313 B) collected in Alabama, Alaska, Florida, Illinois, Iowa, Louisiana, Massachusetts, Michigan, Nevada, New York, North Carolina, Pennsylvania, South Dakota, Virginia and Wisconsin were analyzed for resistance to neuraminidase inhibitors by pyrosequencing assay.
Three (1.4%) of the 211 A(H1N1)pdm09 viruses tested had the H275Y amino acid substitution in the neuraminidase and showed highly reduced inhibition by oseltamivir and peramivir. No molecular markers associated with reduced or highly reduced inhibition by neuraminidase inhibitors were detected in A(H3N2) and type B viruses tested."
HOW MANY PATIENTS WEREN'T EVEN OFFERED ANTIVIRAL MEDICATION AFTER THE CDC 'DIRECTED' THE MEDICAL COMMUNITY TO ASSUME ALL PATIENTS PRESENTING WITH FLU SYMPTOMS WERE PROBABLY COVID-19?
Data cut off Jan. 2020 as COVID-19 CAME TO AMERICA.
WHO Health Emergency Dashboard Disclaimer
"The World Health Organization (WHO) Health Emergency Dashboard is a platform which aims to share information about public health events and emergencies. The data on the dashboard is refreshed every fifteen (15) minutes and data is accurate as at time of refreshing.
The WHO Health Emergency Dashboard is not a comprehensive representation of all the events and emergencies that WHO is aware of and responding to. The events displayed are a subset of those reported through official channels as mandated by the International Health Regulations (IHR 2005).
The content of the WHO Health Emergency Dashboard is for general information only. It is subject to change without notice.
While every reasonable effort has been made to make the information on the WHO Health Emergency Dashboard as timely and accurate as possible, WHO makes no claims, promises or guarantees about the effectiveness, completeness and accuracy of the contents of the WHO Health Emergency Dashboard, and expressly disclaims any liability for damages as a result of the use and/or application of the WHO Health Emergency Dashboard, errors and/or omissions in the content.
The responsibility for the interpretation and use of the content lies with the reader. WHO reserves the right to make updates and changes to posted content without notice and accepts no liability for any errors or omissions in this regard. WHO assumes no responsibility or liability for any consequence resulting directly or indirectly from any action or inaction readers take based on or made in reliance on the information and material available on the WHO Health Emergency Dashboard.
While every reasonable effort has been made to use appropriate language and pictures on the WHO Health Emergency Dashboard, WHO expressly disclaims any responsibility for inadvertent offensive or insensitive, perceived or actual, language or pictures.
WHO will take no responsibility for or be liable for the WHO Health Emergency Dashboard being temporarily unavailable in the event of technical or other issues.
WHO will take no responsibility for or be liable for the WHO Health Emergency Dashboard being temporarily unavailable in the event of technical or other issues.
The size of the pie charts corresponds to the number of events in a given country or territory; the size does not indicate the severity or risk associated with the event(s).
The designations employed and the presentation of content on the WHO Health Emergency Dashboard, including names of the events, maps and other illustrative materials, do not imply the expression of any opinion whatsoever on the part of WHO concerning the legal status of any country, territory, city or area, or of its authorities, or concerning the delineation of frontiers and borders.
Grey areas on maps represent approximate border lines for which there may not yet be full agreement."
THEY COVERED THEIR ASSES QUITE WELL, LEGALLY, DIDN'T THEY?
THERE'S MORE, MUCH MORE, BUT LET THIS SUFFICE AS A BEGINNING TO UNDERSTANDING THAT THIS "CRISIS" WAS MANUFACTURED, MANIPULATED, JUST AS THE AFTERMATH EXCUSE-MAKING OF THE PANIC-DRIVEN SWINE FLU PANDEMIC OF 2009-2010 WAS.
THE WORLD WAS NOT STOPPED IN ITS TRACKS THEN AND SHOULD NOT HAVE BEEN THIS TIME.
THE WRLDWIDE ECONOMY HAS BEEN DEVASTATED BY THIS RECENT FIASCO, BUT NO ONE WILL TAKE WH/CDC TO TASK.
THEY ARE ABOVE THE LAW.
WHO AND CDC DON'T WANT WORLDWIDE RAGE THAT THEY BASED THEIR PREDICTIONS ON ESTIMATES, FAKERY, SKEWED DATA, FLAWED TESTS, CONTAMINATED LABS, ELEVATED DEATH COUNTS BY FRAUDULENT MEANS, ETC.
THEY WILL ESCAPE THE WRATH OF NATIONS THIS TIME JUST AS THEY DID DURING THE SARS, MERS, H1N1 SCARES OF THE PAST.
THEY KNOW THE MASSES WILL ACCEPT THEIR LIES AND FAKE DATA, THEIR EXCUSES AND SO THEY JUST KEEP SPEWING IT.
NEXT YEAR, OR MAYBE EVEN THIS YEAR, THEY WILL RAISE A NEW ALARM OVER A NEWER VIRUS/PANDEMIC AND THE MASSES WILL ONCE AGAIN PANIC AND SUBMIT.
THIS IS WHAT HAPPENS WHEN AVERAGE CITIZENS EITHER HAVE NO MEANS TO FACT-CHECK THE SO-CALLED FACT-CHECKERS, THE DATA-PROVIDERS, THE TEST LABS, THE WHO OR CDC, OR WHEN THE GULLIBLE SHEEP JUST CONTINUOUSLY ACCEPT WHAT THE 'POWERS THAT BE' SAY.
IT SEEMS WE JUST NEVER LEARN.
HATS OFF AND SALUTES TO THOSE WHO ARE SAYING THEY WON'T ENFORCE UNCONSTITUTIONAL RULES DURING THIS MANIPULATED "PANDEMIC".
Racine County Sheriff Christopher Schmaling announced on Friday his department will not be enforcing Wisconsin’s Draconian stay-at-home order.
FOUR COUNTY SHERIFFS WILL NOT ENFORCE MICHIGAN GOVERNOR'S RULES
STATEWIDE PROTESTS ERUPT.
ALABAMA ND TEXAS TO REOPEN THEIR ECONOMY/BUSINESSES.
'Worst Is Over,' Cuomo Says as 7 States Ally to Reopen Economy
https://www.nytimes.com/2020/04/13/nyregion/coronavirus-new-york-update.html
5 days ago.
'Worst Is Over,' Cuomo Says as 7 States Ally to Reopen Economy.


//WW
THEY COVERED THEIR ASSES QUITE WELL, LEGALLY, DIDN'T THEY?
THERE'S MORE, MUCH MORE, BUT LET THIS SUFFICE AS A BEGINNING TO UNDERSTANDING THAT THIS "CRISIS" WAS MANUFACTURED, MANIPULATED, JUST AS THE AFTERMATH EXCUSE-MAKING OF THE PANIC-DRIVEN SWINE FLU PANDEMIC OF 2009-2010 WAS.
THE WORLD WAS NOT STOPPED IN ITS TRACKS THEN AND SHOULD NOT HAVE BEEN THIS TIME.
THE WRLDWIDE ECONOMY HAS BEEN DEVASTATED BY THIS RECENT FIASCO, BUT NO ONE WILL TAKE WH/CDC TO TASK.
THEY ARE ABOVE THE LAW.
WHO AND CDC DON'T WANT WORLDWIDE RAGE THAT THEY BASED THEIR PREDICTIONS ON ESTIMATES, FAKERY, SKEWED DATA, FLAWED TESTS, CONTAMINATED LABS, ELEVATED DEATH COUNTS BY FRAUDULENT MEANS, ETC.
THEY WILL ESCAPE THE WRATH OF NATIONS THIS TIME JUST AS THEY DID DURING THE SARS, MERS, H1N1 SCARES OF THE PAST.
THEY KNOW THE MASSES WILL ACCEPT THEIR LIES AND FAKE DATA, THEIR EXCUSES AND SO THEY JUST KEEP SPEWING IT.
NEXT YEAR, OR MAYBE EVEN THIS YEAR, THEY WILL RAISE A NEW ALARM OVER A NEWER VIRUS/PANDEMIC AND THE MASSES WILL ONCE AGAIN PANIC AND SUBMIT.
THIS IS WHAT HAPPENS WHEN AVERAGE CITIZENS EITHER HAVE NO MEANS TO FACT-CHECK THE SO-CALLED FACT-CHECKERS, THE DATA-PROVIDERS, THE TEST LABS, THE WHO OR CDC, OR WHEN THE GULLIBLE SHEEP JUST CONTINUOUSLY ACCEPT WHAT THE 'POWERS THAT BE' SAY.
IT SEEMS WE JUST NEVER LEARN.
HATS OFF AND SALUTES TO THOSE WHO ARE SAYING THEY WON'T ENFORCE UNCONSTITUTIONAL RULES DURING THIS MANIPULATED "PANDEMIC".
Racine County Sheriff Christopher Schmaling announced on Friday his department will not be enforcing Wisconsin’s Draconian stay-at-home order.
FOUR COUNTY SHERIFFS WILL NOT ENFORCE MICHIGAN GOVERNOR'S RULES
STATEWIDE PROTESTS ERUPT.
ALABAMA ND TEXAS TO REOPEN THEIR ECONOMY/BUSINESSES.
'Worst Is Over,' Cuomo Says as 7 States Ally to Reopen Economy
https://www.nytimes.com/2020/04/13/nyregion/coronavirus-new-york-update.html
5 days ago.
'Worst Is Over,' Cuomo Says as 7 States Ally to Reopen Economy.
//WW
No comments:
Post a Comment